

Surgical Considerations in the Treatment of Ankle Instability
- PMID: 12937567
- PMCID: PMC164377
Surgical Considerations in the Treatment of Ankle Instability
Abstract
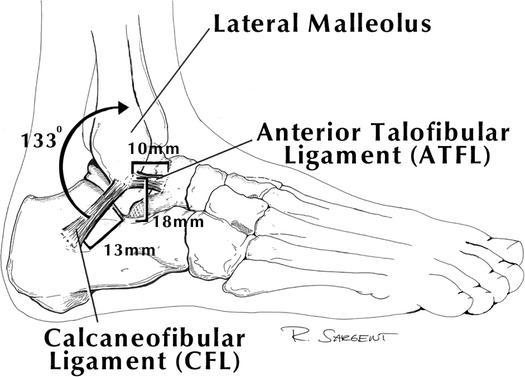
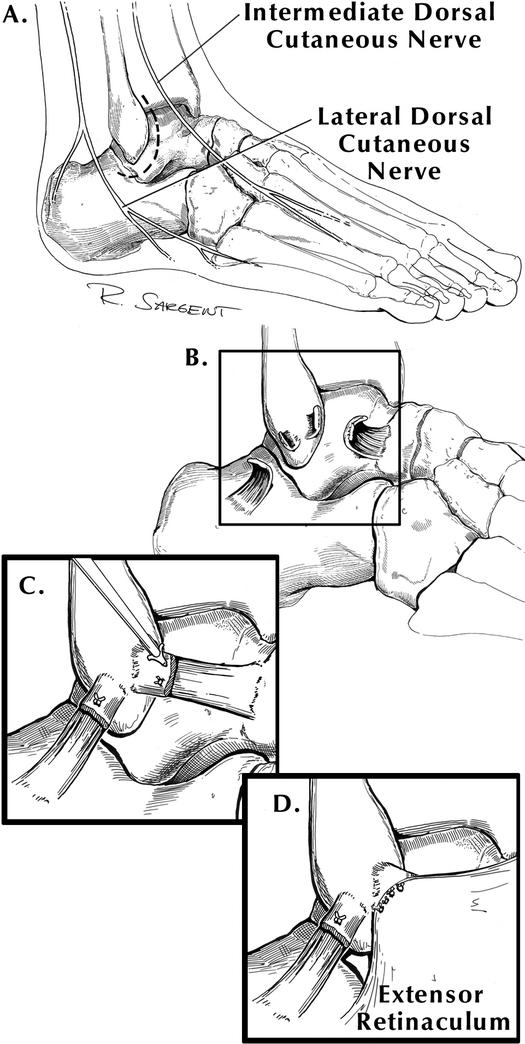
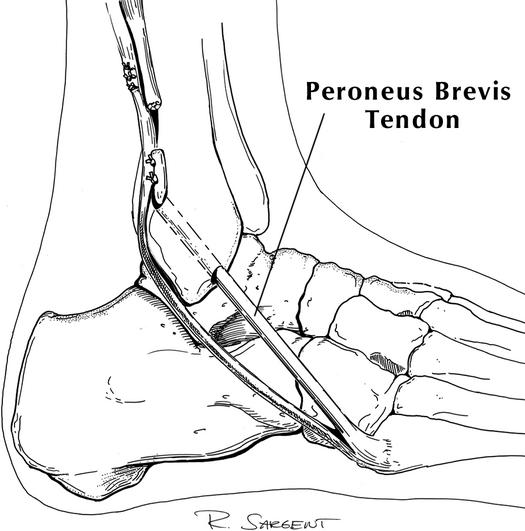
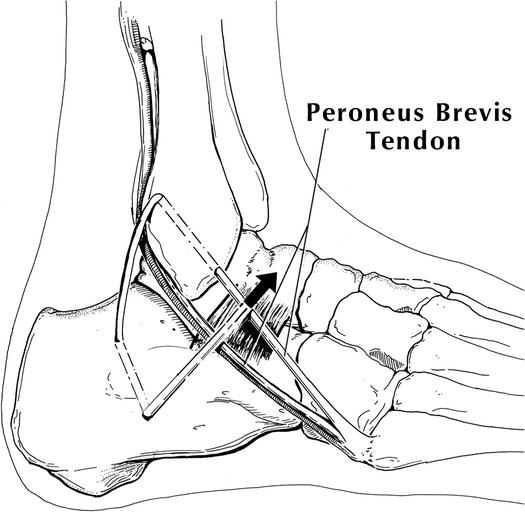
OBJECTIVE: To review the surgical indications, techniques, biomechanical testing, and clinical results reported for the most common surgical techniques used to treat ankle instability. DATA SOURCES: We searched MEDLINE from 1960-2001 using the terms ankle instability, functional ankle instability, mechanical ankle instability, ankle ligament surgery, Broström, Chrisman-Snook, and Evans. DATA SYNTHESIS: Although 80% to 85% of acute ankle sprains are successfully treated with a functional ankle-rehabilitation program, the remaining 15% to 20% have recurrent ankle instability and reinjury, necessitating surgical intervention. The fundamentals of the surgical approach to lateral ankle instability are based on the anatomy of the lateral ankle ligaments, the anterior talofibular ligament, and the calcaneofibular ligament. Ankle-instability surgery has been broadly divided into an anatomic repair consisting of an imbrication of the lateral ligamentous complex and an ankle-ligament reconstruction. An ankle-ligament reconstruction weaves a harvested tendon graft, most commonly the peroneus brevis, to augment the lateral ligaments of the ankle. Goals of surgery are to reestablish ankle stability and function without compromising motion and without complications. Anatomic repair and imbrication of the lateral ligament complex with the Gould modification has an 85% to 95% success rate, and the risk of associated nerve injuries is low. This approach provides increased stability by reinforcing local host tissue, preserving subtalar and talocrural motion, eliminating the comorbidity associated with tendon-graft harvest, and offering a quicker functional recovery. One concern in using the anatomic approach is the resultant strength of the repair, although the literature does not support this concern. Ankle-reconstruction procedures that sacrifice tendons are thought to provide a stronger construct, and hence, more stability. This increased stability results in loss of talocrural and subtalar range of motion, prolonging recovery and decreasing sport performance. Adjacent nerve injury is more common with ankle-ligament reconstruction. CONCLUSIONS/RECOMMENDATIONS: Based on the literature, we believe that a modified Broström lateral-ligament repair should be considered the first choice for persistent ankle instability refractory to a functional ankle-rehabilitation protocol. Ankle reconstruction with tendon augmentation should be reserved for patients with generalized ligamentous laxity or long-standing ligamentous insufficiency or as a salvage procedure in a patient with a failed modified Broström lateral-ligament repair.
Figures
References
-
- Colville M R, Marder R A, Boyle J J, Zarins B. Strain measurement in lateral ankle ligaments. Am J Sports Med. 1990;18:196–200. - PubMed
-
- Burks R T, Morgan J. Anatomy of the lateral ankle ligaments. Am J Sports Med. 1994;22:72–77. - PubMed
-
- Colville M R. Surgical treatment of the unstable ankle. J Am Acad Orthop Surg. 1998;6:368–377. - PubMed
-
- Heilman A E, Braly W G, Bishop J O, Noble P C, Tullos H S. An anatomic study of subtalar instability. Foot Ankle. 1990;10:224–228. - PubMed
-
- Broström L. Sprained ankles, VI: surgical treatment of “chronic” ligament ruptures. Acta Chir Scand. 1966;243:551–565. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources