

Strain and strain rate parametric imaging. A new method for post processing to 3-/4-dimensional images from three standard apical planes. Preliminary data on feasibility, artefact and regional dyssynergy visualisation
- PMID: 12956886
- PMCID: PMC194434
- DOI: 10.1186/1476-7120-1-11
Strain and strain rate parametric imaging. A new method for post processing to 3-/4-dimensional images from three standard apical planes. Preliminary data on feasibility, artefact and regional dyssynergy visualisation
Abstract
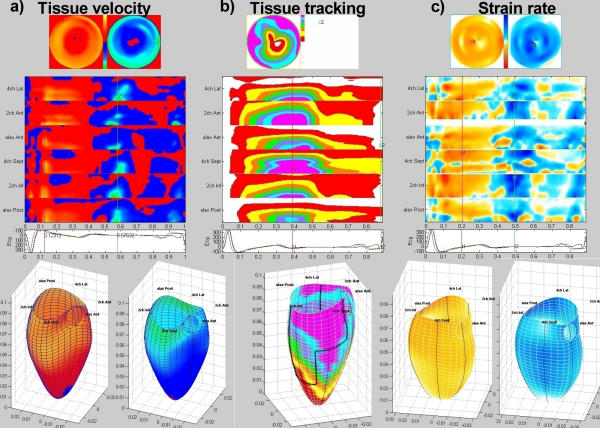
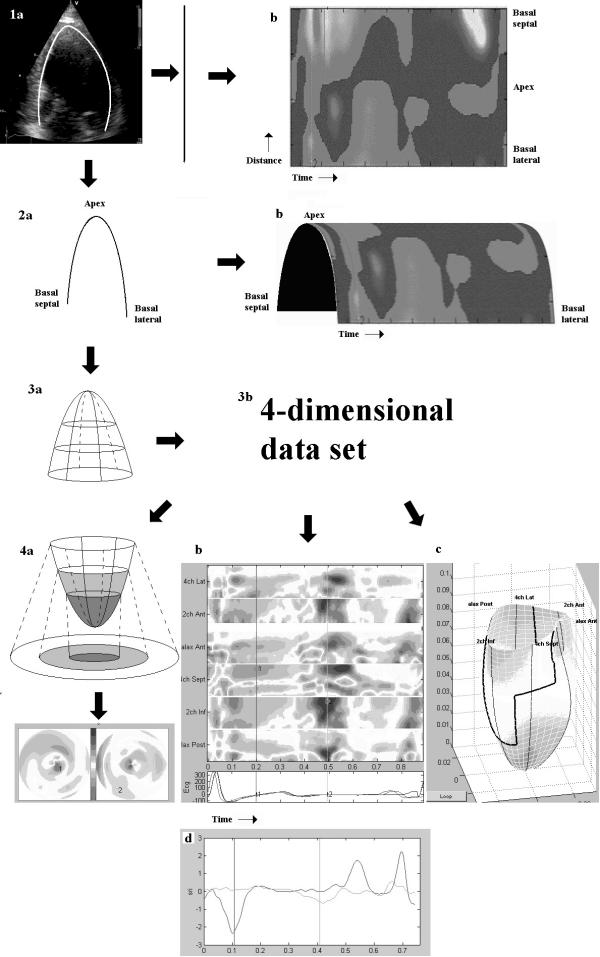
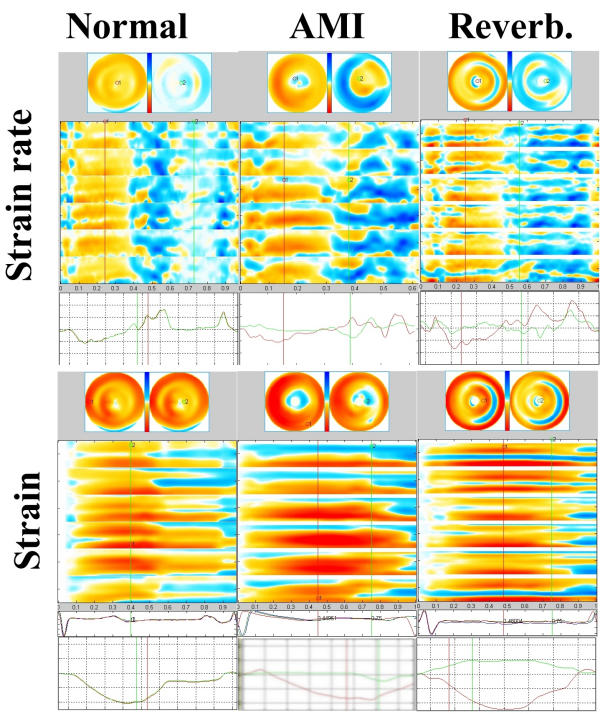
Background: We describe a method for 3-/4D reconstruction of tissue Doppler data from three standard apical planes, post processing to derived data of strain rate/strain and parametric colour imaging of the data. The data can be displayed as M-mode arrays from all six walls, Bull's eye projection and a 3D surface figure that can be scrolled and rotated. Numerical data and waveforms can be re-extracted.
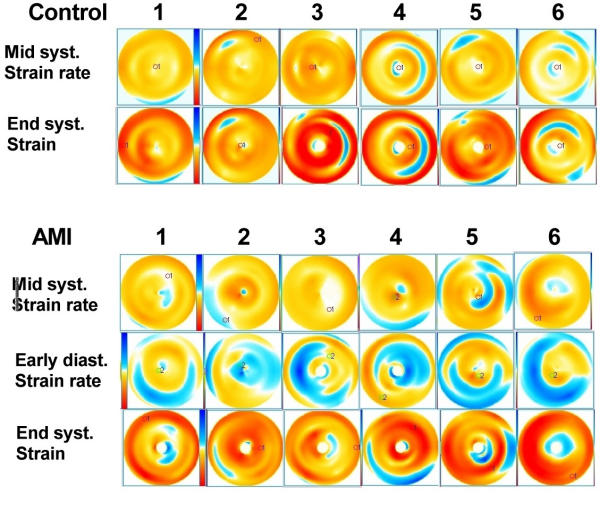
Methods: Feasibility was tested by Strain Rate Imaging in 6 normal subjects and 6 patients with acute myocardial infarction. Reverberation artefacts and dyssynergy was identified by colour images. End systolic strain, peak systolic and mid systolic strain rate were measured.
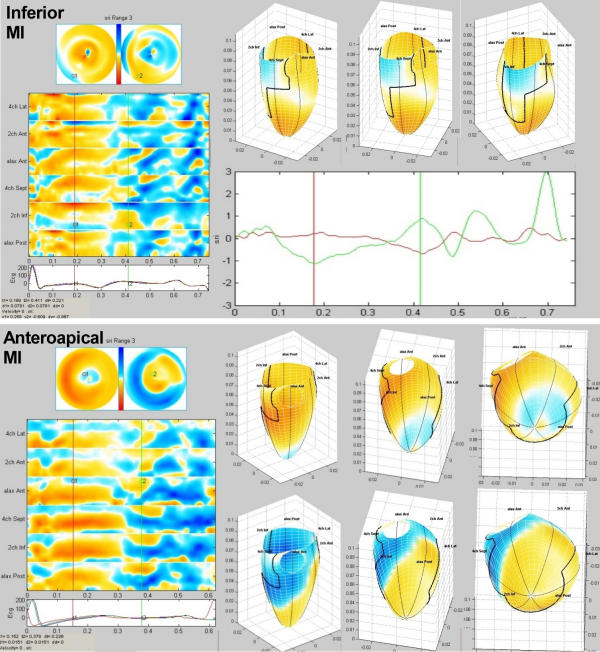
Results: Infarcts were visualised in all patients by colour imaging of mid systolic strain rate, end systolic strain and post systolic shortening by strain rate. Reverberation artefacts were visible in 3 of 6 normals, and 2 of 6 patients, and were identified both on bull's eye and M-mode display, but influenced quantitative measurement. Peak systolic strain rate was in controls minimum -1.11, maximum -0.89 and in patients minimum -1.66, maximum 0.02 (p = 0.04). Mid systolic strain rate and end systolic strain did not separate the groups significantly.
Conclusion: 3-/4D reconstruction and colour display is feasible, allowing quick visual identification of infarcts and artefacts, as well as extension of area of post systolic shortening. Strain rate is better suited to colour parametric display than strain.
Figures
Similar articles
-
Velocity tracking, a new and user independent method for detecting regional function of the left ventricle.Clin Physiol Funct Imaging. 2009 Jan;29(1):24-31. doi: 10.1111/j.1475-097X.2008.00828.x. Epub 2008 Sep 24. Clin Physiol Funct Imaging. 2009. PMID: 18823334
-
Three-dimensional principal strain analysis for characterizing subclinical changes in left ventricular function.J Am Soc Echocardiogr. 2014 Oct;27(10):1041-1050.e1. doi: 10.1016/j.echo.2014.05.014. Epub 2014 Jul 4. J Am Soc Echocardiogr. 2014. PMID: 24998517 Clinical Trial.
-
Novel simple approach for detection of regional perturbations of cardiac function in mouse models of cardiovascular disease.Echocardiography. 2013 Aug;30(7):843-9. doi: 10.1111/echo.12138. Epub 2013 Jan 25. Echocardiography. 2013. PMID: 23346940
-
Non-Doppler two-dimensional strain imaging by echocardiography--from technical considerations to clinical applications.J Am Soc Echocardiogr. 2007 Mar;20(3):234-43. doi: 10.1016/j.echo.2006.08.023. J Am Soc Echocardiogr. 2007. PMID: 17336748 Review.
-
Incoherent artefact correction using PPI.NMR Biomed. 2006 May;19(3):362-7. doi: 10.1002/nbm.1045. NMR Biomed. 2006. PMID: 16705637 Review.
Cited by
-
Heart Performance Determination by Visualization in Larval Fishes: Influence of Alternative Models for Heart Shape and Volume.Front Physiol. 2017 Jul 4;8:464. doi: 10.3389/fphys.2017.00464. eCollection 2017. Front Physiol. 2017. PMID: 28725199 Free PMC article.
-
Three-dimensional mapping of mechanical activation patterns, contractile dyssynchrony and dyscoordination by two-dimensional strain echocardiography: rationale and design of a novel software toolbox.Cardiovasc Ultrasound. 2008 May 30;6:22. doi: 10.1186/1476-7120-6-22. Cardiovasc Ultrasound. 2008. PMID: 18513412 Free PMC article.
-
Wave propagation of myocardial stretch: correlation with myocardial stiffness.Basic Res Cardiol. 2014;109(6):438. doi: 10.1007/s00395-014-0438-5. Epub 2014 Sep 6. Basic Res Cardiol. 2014. PMID: 25193091 Free PMC article.
-
Phase rotation methods in filtering correlation coefficients for ultrasound speckle tracking.IEEE Trans Ultrason Ferroelectr Freq Control. 2009 Jul;56(7):1368-82. doi: 10.1109/TUFFC.2009.1193. IEEE Trans Ultrason Ferroelectr Freq Control. 2009. PMID: 19574148 Free PMC article.
References
-
- Sutherland GR, Stewart MJ, Groundstroem KW, Moran CM, Fleming A, Guell-Peris FJ, Riemersma RA, Fenn LN, Fox KA, McDicken WN. Color Doppler myocardial imaging: a new technique for the assessment of myocardial function. J Am Soc Echocardiogr. 1994;7:441–58. - PubMed
-
- Höglund C, Alam M, Thorstrand C. Atrioventricular valve plane displacement in healthy persons. An echocardiographic study. Acta Med Scand. 1988;224:557–562. - PubMed
-
- Simonson JS, Schiller NB. Descent of the base of the left ventricle: an echocardiographic index of left ventricular function. J Am Soc Echocardiogr. 1989;2:25–35. - PubMed
-
- Alam M, Hoglund C, Thorstrand C. Longitudinal systolic shortening of the left ventricle: an echocardiographic study in subjects with and without preserved global function. Clin Physiol. 1992;12:443–52. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
