

Identifying physician-recognized depression from administrative data: consequences for quality measurement
- PMID: 12968818
- PMCID: PMC1360934
- DOI: 10.1111/1475-6773.00164
Identifying physician-recognized depression from administrative data: consequences for quality measurement
Abstract
Background: Multiple factors limit identification of patients with depression from administrative data. However, administrative data drives many quality measurement systems, including the Health Plan Employer Data and Information Set (HEDIS).
Methods: We investigated two algorithms for identification of physician-recognized depression. The study sample was drawn from primary care physician member panels of a large managed care organization. All members were continuously enrolled between January 1 and December 31, 1997. Algorithm 1 required at least two criteria in any combination: (1) an outpatient diagnosis of depression or (2) a pharmacy claim for an antidepressant Algorithm 2 included the same criteria as algorithm 1, but required a diagnosis of depression for all patients. With algorithm 1, we identified the medical records of a stratified, random subset of patients with and without depression (n = 465). We also identified patients of primary care physicians with a minimum of 10 depressed members by algorithm 1 (n = 32,819) and algorithm 2 (n = 6,837).
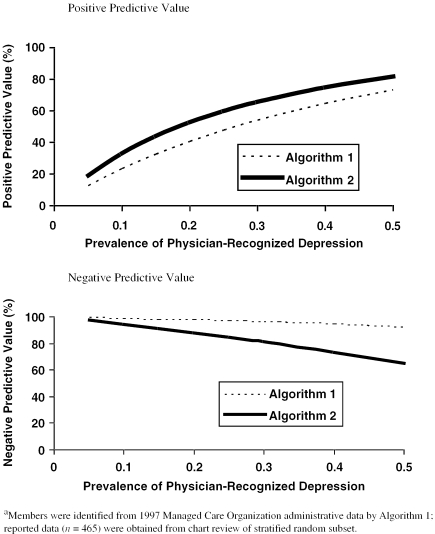
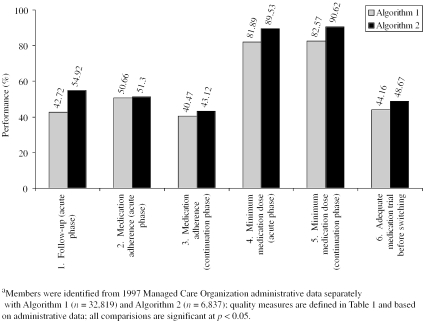
Results: The sensitivity, specificity, and positive predictive values were: Algorithm 1: 95 percent, 65 percent, 49 percent; Algorithm 2: 52 percent, 88 percent, 60 percent. Compared to algorithm 1, profiles from algorithm 2 revealed higher rates of follow-up visits (43 percent, 55 percent) and appropriate antidepressant dosage acutely (82 percent, 90 percent) and chronically (83 percent, 91 percent) (p < 0.05 for all).
Conclusions: Both algorithms had high false positive rates. Denominator construction (algorithm 1 versus 2) contributed significantly to variability in measured quality. Our findings raise concern about interpreting depression quality reports based upon administrative data.
Figures
Similar articles
-
Impact of disseminating quality improvement programs for depression in managed primary care: a randomized controlled trial.JAMA. 2000 Jan 12;283(2):212-20. doi: 10.1001/jama.283.2.212. JAMA. 2000. PMID: 10634337 Clinical Trial.
-
Are there detectable differences in quality of care or outcome of depression across primary care providers?Med Care. 2000 Jun;38(6):552-61. doi: 10.1097/00005650-200006000-00002. Med Care. 2000. PMID: 10843308
-
HEDIS antidepressant medication management measures and performance-based measures: an opportunity for improvement in depression care.Am J Manag Care. 2007 Nov;13(4 Suppl):S98-102. Am J Manag Care. 2007. PMID: 18041869 Review.
-
Collaborative management to achieve treatment guidelines. Impact on depression in primary care.JAMA. 1995 Apr 5;273(13):1026-31. JAMA. 1995. PMID: 7897786 Clinical Trial.
-
NCQA behavioral health measurement efforts.J Manag Care Pharm. 2005 Apr;11(3 Suppl):S9-11. doi: 10.18553/jmcp.2005.11.3.s9. J Manag Care Pharm. 2005. PMID: 15804202 Free PMC article. Review.
Cited by
-
Tribute to John M. Eisenberg.Health Serv Res. 2003 Aug;38(4):993-8. doi: 10.1111/1475-6773.00158. Health Serv Res. 2003. PMID: 14524347 Free PMC article. No abstract available.
-
Capturing Information About Multiple Sclerosis Comorbidity Using Clinical Interviews and Administrative Records: Do the Data Sources Agree?Healthcare (Basel). 2025 May 28;13(11):1281. doi: 10.3390/healthcare13111281. Healthcare (Basel). 2025. PMID: 40508894 Free PMC article.
-
Ten-year trends in quality of care and spending for depression: 1996 through 2005.Arch Gen Psychiatry. 2011 Dec;68(12):1218-26. doi: 10.1001/archgenpsychiatry.2011.146. Arch Gen Psychiatry. 2011. PMID: 22147841 Free PMC article.
-
Medication use and spending trends among children with ADHD in Florida's Medicaid program, 1996-2005.Psychiatr Serv. 2012 Feb 1;63(2):115-21. doi: 10.1176/appi.ps.201100095. Psychiatr Serv. 2012. PMID: 22302327 Free PMC article.
-
Depression in adults with sickle cell disease: a systematic review of the methodological issues in assessing prevalence of depression.BMC Psychol. 2021 Apr 6;9(1):54. doi: 10.1186/s40359-021-00543-4. BMC Psychol. 2021. PMID: 33823930 Free PMC article.
References
-
- Agency for Health Care Policy and Research . Depression in Primary Care: Treatment of Major Depression. Rockville, MD: Agency for Health Care Policy and Research; 1993.
-
- Allison JJ, Calhoun JW, Wall TC, Spettell CM, Fargason CA, Weissman NW, Kiefe CI. “Optimal Reporting of Health Care Process Measures: Inferential Statistics as Help or Hindrance?”. Managed Care Quarterly. 2000;8(4):1–10. - PubMed
-
- Allison JJ, Wall TC, Spettell CM, Calhoun J, Fargason CA, Kobylinski R, Farmer R, Kiefe CI. “The Art and Science of Chart Review.”. Joint Commission Journal on Quality Improvement. 2000;26(3):115–36. - PubMed
-
- American Psychiatric Association . Diagnostic and Statistical Manual of Mental Disorders. 4th Edition. Washington, DC: American Psychiatric Association; 1994.
-
- Badger LW, deGruy FV, Hartman J, Plant MA, Leeper J, Ficken R, Maxwell A, Rand E, Anderson R, Templeton B. “Psychosocial Interest, Medical Interviews, and the Recognition of Depression.”. Archives of Family Medicine. 1994;3(10):899–907. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
