

Population pharmacokinetics and pharmacodynamics of enoxaparin in unstable angina and non-ST-segment elevation myocardial infarction
- PMID: 12968985
- PMCID: PMC1884380
- DOI: 10.1046/j.1365-2125.2003.01904.x
Population pharmacokinetics and pharmacodynamics of enoxaparin in unstable angina and non-ST-segment elevation myocardial infarction
Abstract
Aims: A major concern with any antithrombotic therapy is an increase in the risk of haemorrhage. The aim of this study was to analyse population pharmacokinetics and pharmacokinetic/pharmacodynamic (PK/PD) relationships for enoxaparin in patients with unstable angina (UA) and non-ST-segment elevation myocardial infarction (NSTEMI), which may help predict risk of haemorrhage.
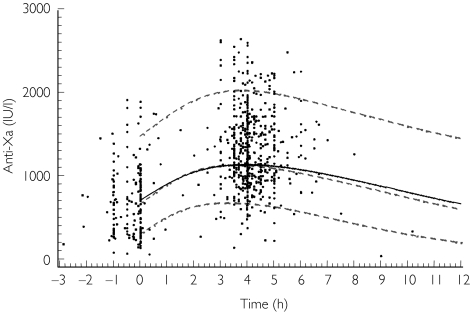
Methods: Anti-factor Xa (anti-Xa) activity was measured as marker of enoxaparin concentration in 448 patients receiving the drug as a single 30-mg intravenous bolus followed by 1.0 or 1.25 mg kg(-1) subcutaneously twice a day. A population pharmacokinetic analysis was conducted and individual estimates of enoxaparin clearance and area under the curve were tested as prognostic factors for the occurrence of haemorrhagic episodes.
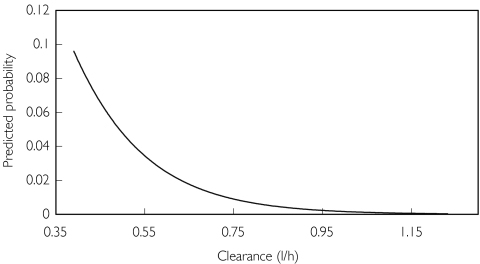
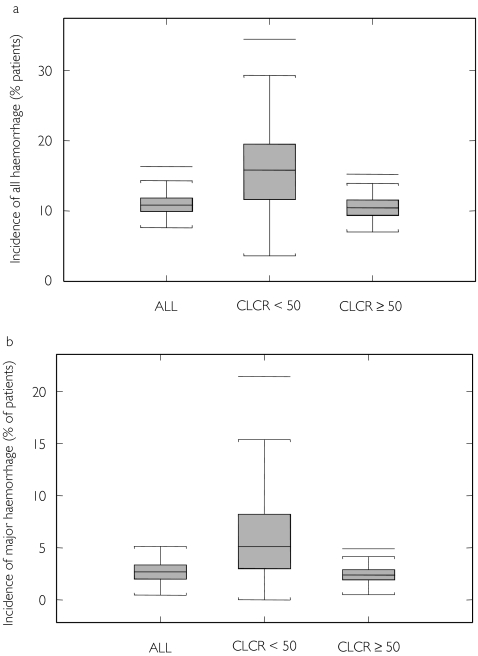
Results: Basic population PK parameters were an enoxaparin clearance of 0.733 l h(-1)[95% confidence interval (CI) 0.698, 0.738], a distribution volume of 5.24 l (95% CI 4.20, 6.28) and an elimination half-life of 5.0 h. Enoxaparin clearance was significantly related to patient weight and creatinine clearance, and was the only independent predictor of experiencing both all (10.7%, P = 0.0013) and major (2.2%, P = 0.0004) haemorrhagic events. A creatinine clearance of 30 ml min(-1) was associated with a decrease in enoxaparin clearance of 27% compared with that in a patient with a median creatinine clearance of 88 ml min-1, and was related to a 1.5- and 3.8-fold increase in the risk of 'all' and 'major' haemorrhagic episodes, respectively.
Conclusions: Enoxaparin clearance depends on body weight, and, therefore, weight-adjusted dosing is recommended to minimize interpatient variability in drug exposure and the risk of haemorrhage. The importance of an increased risk of haemorrhage with decreasing renal function must be weighed against the benefit of treatment with enoxaparin in patients with UA and NSTEMI.
Figures
References
-
- Thrombolysis in Myocardial Infarction (TIMI) 11A Trial Investigators. Dose-ranging trial of enoxaparin for unstable angina: results of TIMI 11A. J Am Coll Cardiol. 1997;29:1474–1482. - PubMed
-
- Antman EM, McCabe CH, Gurfinkel EP, et al. Enoxaparin prevents death and cardiac ischemic events in unstable angina/non-Q-wave myocardial infarction. Results of the thrombolysis in myocardial infarction (TIMI) 11B trial. Circulation. 1999;100:1593–1601. - PubMed
-
- Beal SL, Boeckman AJ, Sheiner LB. NONMEM user's guide, Parts I-VII. San Francisco: University of California at San Francisco; 1988. 1992.
-
- Karlsson MO, Sheiner LB. The importance of modelling interoccasion variability in population pharmacokinetic analyses. J Pharmacokinet Biopharm. 1993;21:735–750. - PubMed
-
- Beal SL. Validation of a population model. E-mail on the NONMEM Users Network. 1994. http://www.phor.com/nonmem/nmo/topic006.html. 1 February.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
