

Safety and efficacy of factor IX gene transfer to skeletal muscle in murine and canine hemophilia B models by adeno-associated viral vector serotype 1
- PMID: 12969984
- PMCID: PMC4704086
- DOI: 10.1182/blood-2003-05-1446
Safety and efficacy of factor IX gene transfer to skeletal muscle in murine and canine hemophilia B models by adeno-associated viral vector serotype 1
Abstract
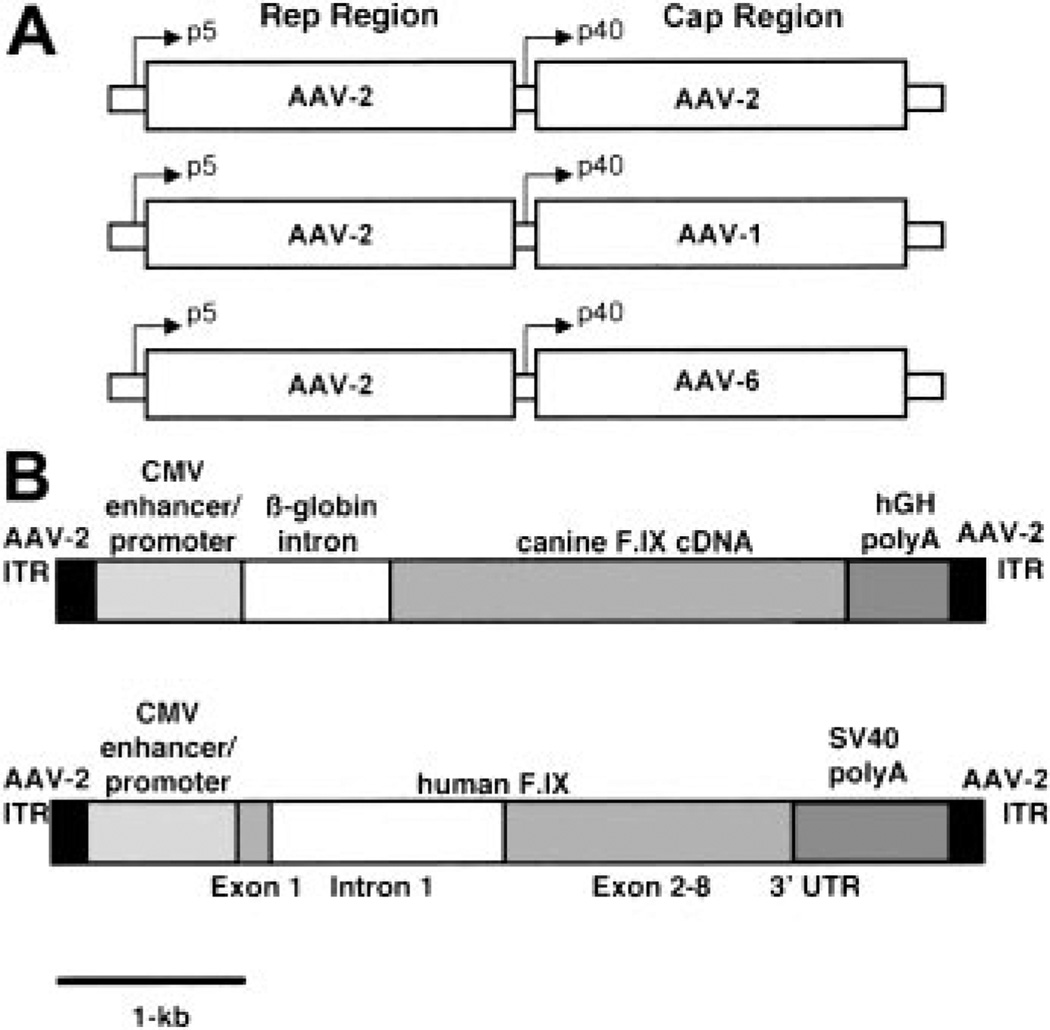
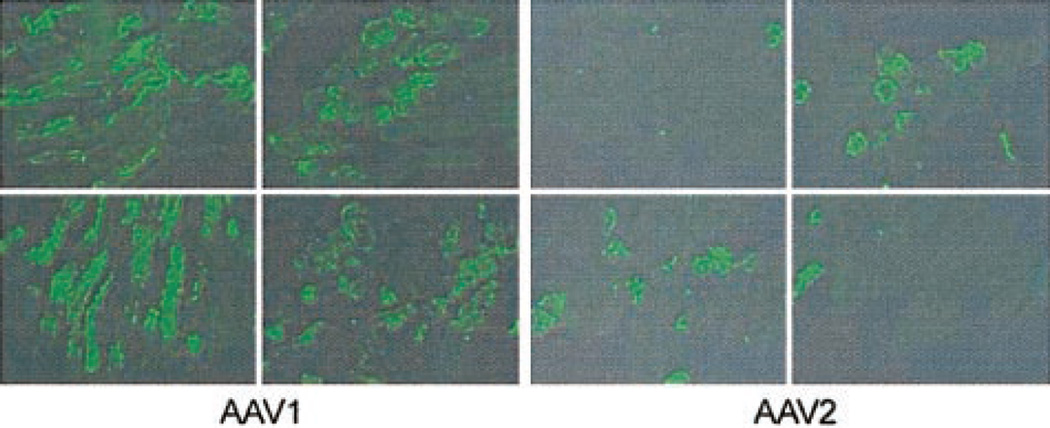
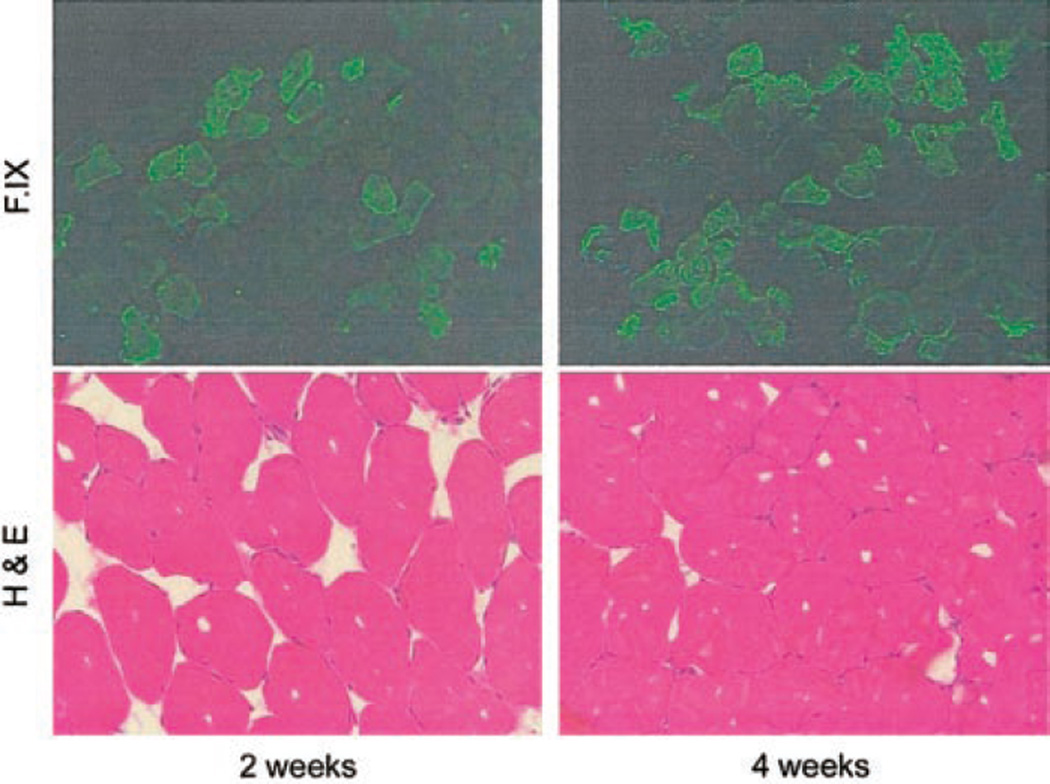
Adeno-associated viral (AAV) vectors (serotype 2) efficiently transduce skeletal muscle, and have been used as gene delivery vehicles for hemophilia B and for muscular dystrophies in experimental animals and humans. Recent reports suggest that AAV vectors based on serotypes 1, 5, and 7 transduce murine skeletal muscle much more efficiently than AAV-2, with reported increases in expression ranging from 2-fold to 1000-fold. We sought to determine whether this increased efficacy could be observed in species other than mice. In immunodeficient mice we saw 10- to 20-fold higher levels of human factor IX (hF.IX) expression at a range of doses, and in hemophilic dogs we observed approximately 50-fold higher levels of expression. The increase in transgene expression was due partly to higher gene copy number and a larger number of cells transduced at each injection site. In all immunocompetent animals injected with AAV-1, inhibitory antibodies to F.IX developed, but in immunocompetent mice treated with high doses of vector, inhibitory antibodies eventually disappeared. These studies emphasize that the increased efficacy of AAV-1 vectors carries a risk of inhibitor formation, and that further studies will be required to define doses and treatment regimens that result in tolerance rather than immunity to F.IX.
Figures





References
-
- Wagner JA, Moran ML, Messner AH, et al. A phase I/II study of tgAAV-CF for the treatment of chronic sinusitis in patients with cystic fibrosis. Hum Gene Ther. 1998;9:889–909. - PubMed
-
- Manno CS, Chew AJ, Hutchison S, et al. AAV-mediated factor IX gene transfer to skeletal muscle in patients with severe hemophilia B. Blood. 2003;101:2963–2972. - PubMed
-
- Stedman H, Wilson JM, Finke R, Kleckner AL, Mendell J. Phase I clinical trial utilizin gene therapy for limb girdle muscular dystrophy: alpha-, beta-, gamma-, or delta-sarcoglycan gene delivered with intramuscular instillations of adeno- associated vectors. Hum Gene Ther. 2000;11:777–790. - PubMed
-
- Chao H, Liu Y, Rabinowitz J, Li C, Samulski RJ, Walsh CE. Several log increase in therapeutic transgene delivery by distinct adeno-associated viral serotype vectors. Mol Ther. 2000;2:619–623. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Research Materials
Miscellaneous
