

Evaluation of a prison outreach clinic for the diagnosis and prevention of hepatitis C: implications for the national strategy
- PMID: 12970145
- PMCID: PMC1773842
- DOI: 10.1136/gut.52.10.1500
Evaluation of a prison outreach clinic for the diagnosis and prevention of hepatitis C: implications for the national strategy
Abstract
Background: Hepatitis C virus (HCV) infection is a major public health problem recognised by the UK National Strategy that proposes that a care pathway for assessment, diagnosis, and treatment be established in all prisons, integrated within managed clinical networks. A prison sentence provides the opportunity to focus on traditionally hard to reach patients.
Aims: To evaluate the prevalence of HCV infection in a UK prison cluster and to assess the effectiveness of a prison outreach service for hepatitis C.
Subjects: Male prisoners.
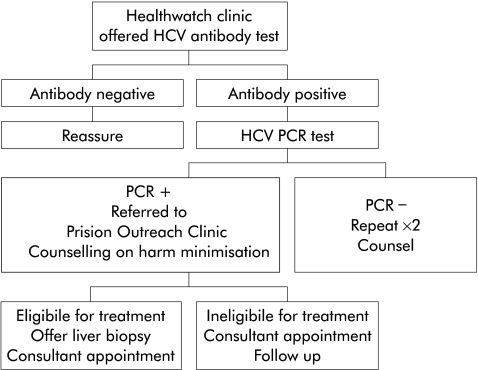
Methods: A nurse specialist led clinic within a cluster of adult prisons was established, offering health education on hepatitis C, advice on harm minimisation, and HCV testing. Infected prisoners were offered access to a care pathway leading to treatment. Outcome measures were uptake of the service, and diagnosis and treatment of hepatitis C.
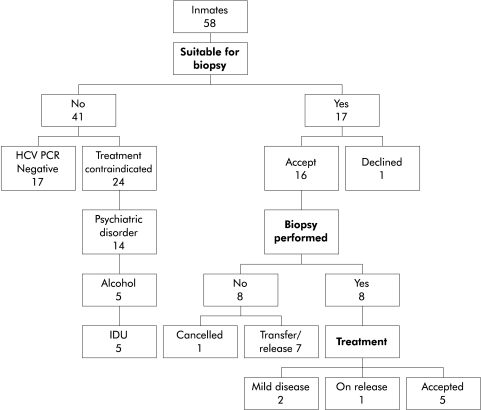
Results: A total of 8.5% of 1618 prisoners accepted testing: 30% had active infection with HCV. Most were ineligible for treatment due to psychiatric illness or did not receive treatment for logistic reasons. Injecting drug use was the major risk factor in all cases. Only 7% of HCV polymerase chain amplification positive inmates received treatment in prison.
Conclusion: There is a large pool of HCV infected prisoners at risk of complications, constituting a source of infection during their sentence and after discharge. A prison outreach clinic and care pathway was perceived as effective in delivering health education, reducing the burden on prison and hospital services. It provided an opportunity for intervention but had a limited effect in eradicating HCV in prisoners and it remains unclear how this might be achieved.
Figures
Comment in
-
In search of the correct strategy for preventing the spread of HCV infection.Gut. 2004 May;53(5):771-2. Gut. 2004. PMID: 15082602 Free PMC article. No abstract available.
References
-
- Department of Health. Hepatitis C Strategy for England, 2002. http://www.doh.gov.uk/cmo/hcvstrategy/77097dhhepcstrat.pdf (accessed 14 July 2003).
-
- Atrah HI, Ala FA, Ahmed MM, et al. Unexplained hepatitis C virus antibody seroconversion in established blood donors. Transfusion 1996;36:339–43. - PubMed
-
- Crofts N, Hopper JL, Milner R, et al. Blood-borne virus infections among Australian injecting drug users: implications for spread of HIV. Eur J Epidemiol 1994;10:687–94. - PubMed
-
- Goldberg D, Cameron S, McMenamin J. Hepatitis C virus antibody prevalence among injecting drug users in Glasgow has fallen but remains high. Commun Dis Public Health 1998;1:95–7. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical