

Increased circulating pro-brain natriuretic peptide (proBNP) and brain natriuretic peptide (BNP) in patients with cirrhosis: relation to cardiovascular dysfunction and severity of disease
- PMID: 12970147
- PMCID: PMC1773816
- DOI: 10.1136/gut.52.10.1511
Increased circulating pro-brain natriuretic peptide (proBNP) and brain natriuretic peptide (BNP) in patients with cirrhosis: relation to cardiovascular dysfunction and severity of disease
Abstract
Background and aims: Cardiac dysfunction may be present in patients with cirrhosis. This study was undertaken to relate plasma concentrations of cardiac peptides reflecting early ventricular dysfunction (pro-brain natriuretic peptide (proBNP) and brain natriuretic peptide (BNP)) to markers of severity of liver disease, cardiac dysfunction, and hyperdynamic circulation in patients with cirrhosis.
Patients and methods: Circulating levels of proBNP and BNP were determined in 51 cirrhotic patients during a haemodynamic investigation.
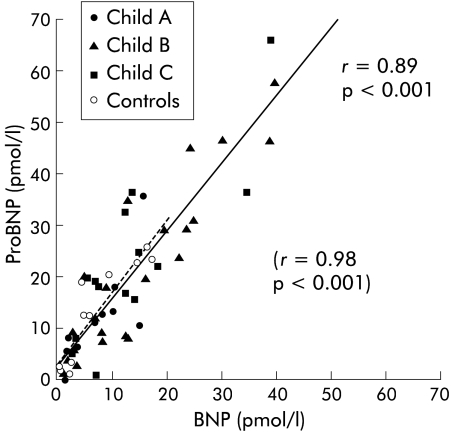
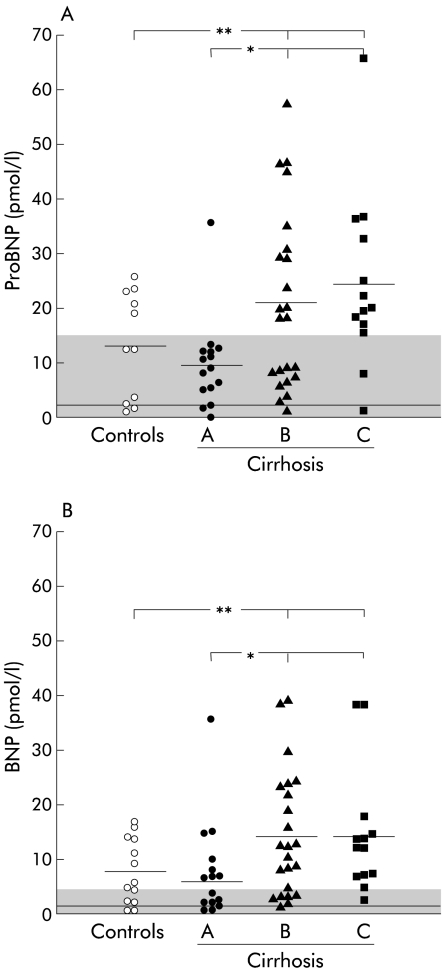
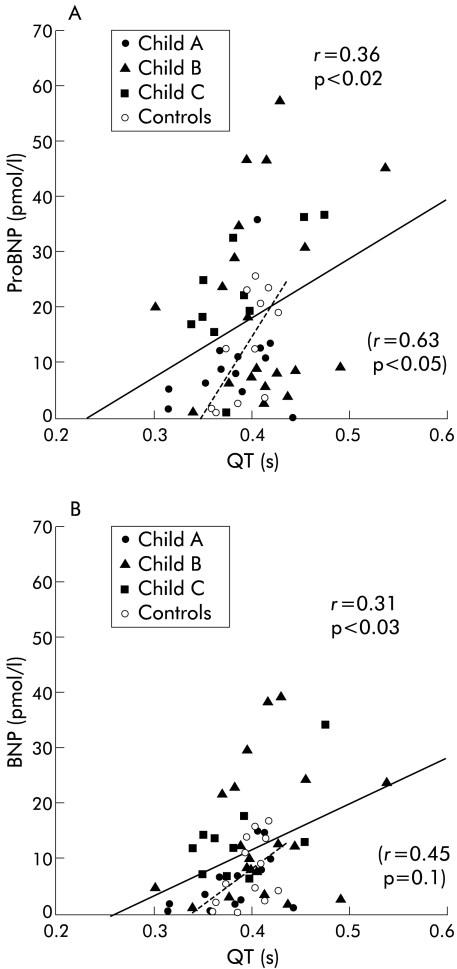
Results: Plasma proBNP and BNP were significantly increased in cirrhotic patients (19 and 12 pmol/l, respectively) compared with age matched controls (14 and 6 pmol/l; p<0.02) and healthy subjects (<15 and <5.3 pmol/l; p<0.002). Circulating proBNP and BNP were closely correlated (r = 0.89, p<0.001), and the concentration ratio proBNP/BNP was similar to that of control subjects (1.8 v 2.3; NS). Circulating proBNP and BNP were related to severity of liver disease (Child score, serum albumin, coagulation factors 2, 7, and 10, and hepatic venous pressure gradient) and to markers of cardiac dysfunction (QT interval, heart rate, plasma volume) but not to indicators of the hyperdynamic circulation. Moreover, in multiple regression analysis, proBNP and BNP were also related to arterial carbon dioxide and oxygen tensions. The rate of hepatic disposal of proBNP and BNP was not significantly different in cirrhotic patients and controls.
Conclusion: Elevated circulating levels of proBNP and BNP in patients with cirrhosis most likely reflects increased cardiac ventricular generation of these peptides and thus indicates the presence of cardiac dysfunction, rather than being caused by the hyperdynamic circulatory changes found in these patients.
Figures
Comment in
-
Origins of cardiac dysfunction in cirrhosis.Gut. 2003 Oct;52(10):1392-4. doi: 10.1136/gut.52.10.1392. Gut. 2003. PMID: 12970127 Free PMC article. No abstract available.
References
-
- Schrier RW, Arroyo V, Bernardi M, et al. Peripheral artery vasodilatation hypotheses: a proposal for the initiation of renal sodium and water retention in cirrhosis. Hepatology 1988;8:1151–7. - PubMed
-
- Møller S, Henriksen JH. Circulatory abnormalities in cirrhosis with focus on neurohumoral aspects. Semin Nephrol 1997;17:505–19. - PubMed
-
- Naschitz JE, Slobodin G, Lewis RJ, et al. Heart diseases affecting the liver and liver diseases affecting the heart. Am Heart J 2000;140:111–20. - PubMed
-
- Estruch R, Fernandezsola J, Sacanella E, et al. Relationship between cardiomyopathy and liver disease in chronic alcoholism. Hepatology 1995;22:532–8. - PubMed
-
- Pozzi M, Carugo S, Boari G, et al. Evidence of functional and structural cardiac abnormalities in cirrhotic patients with and without ascites. Hepatology 1997;26:1131–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous