

The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care
- PMID: 12975221
- PMCID: PMC191278
The medical office of the 21st century (MOXXI): effectiveness of computerized decision-making support in reducing inappropriate prescribing in primary care
Abstract
Background: Adverse drug-related events are common in the elderly, and inappropriate prescribing is a preventable risk factor. Our objective was to determine whether inappropriate prescribing could be reduced when primary care physicians had computer-based access to information on all prescriptions dispensed and automated alerts for potential prescribing problems.
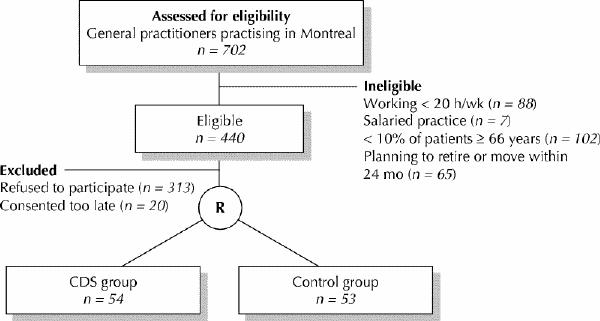
Methods: We randomly assigned 107 primary care physicians with at least 100 patients aged 66 years and older (total 12 560) to a group receiving computerized decision-making support (CDS) or a control group. Physicians in the CDS group had access to information on current and past prescriptions through a dedicated computer link to the provincial seniors' drug-insurance program. When any of 159 clinically relevant prescribing problems were identified by the CDS software, the physician received an alert that identified the nature of the problem, possible consequences and alternative therapy. The rate of initiation and discontinuation of potentially inappropriate prescriptions was assessed over a 13-month period.
Results: In the 2 months before the study, 31.8% of the patients in the CDS group and 33.3% of those in the control group had at least 1 potentially inappropriate prescription. During the study the number of new potentially inappropriate prescriptions per 1000 visits was significantly lower (18%) in the CDS group than in the control group (relative rate [RR] 0.82, 95% confidence interval [CI] 0.69-0.98), but differences between the groups in the rate of discontinuation of potentially inappropriate prescriptions were significant only for therapeutic duplication by the study physician and another physician (RR 1.66, 95% CI 0.99-2.79) and drug interactions caused by prescriptions written by the study physician (RR 2.15, 95% CI 0.98-4.70).
Interpretation: Computer-based access to complete drug profiles and alerts about potential prescribing problems reduces the rate of initiation of potentially inappropriate prescriptions but has a more selective effect on the discontinuation of such prescriptions.
Figures
References
-
- Lazarou J, Pomeranz BH, Corey PN. Incidence of adverse drug reactions in hospitalized patients: a meta-analysis of prospective studies. JAMA 1998;279:1200-5. - PubMed
-
- Hallas J, Harvald B, Gram LF, Grodum E, Brosen K, Haghfelt T. Drug related hospital admissions: the role of definitions and intensity of data collection, and the possibility of prevention. J Intern Med 1990;228:83-90. - PubMed
-
- Colt HG, Shapiro AP. Drug-induced illness as a cause for admission to a community hospital. J Am Geriatr Soc 1989;37:323-6. - PubMed
-
- Ives TJ, Bentz EJ, Gwyther RE. Drug-related admissions to a family medicine inpatient service. Arch Intern Med 1987;147:1117-20. - PubMed
-
- Jha A, Kuperman GJ, Rittenberg E, Teich JM, Bates DW. Identifying hospital admissions due to adverse drug events using a computer-based monitor. Pharmacoepidemiol Drug Saf 2001;10:113-9. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous