

Effects of isolated obesity on systolic and diastolic left ventricular function
- PMID: 12975404
- PMCID: PMC1767886
- DOI: 10.1136/heart.89.10.1152
Effects of isolated obesity on systolic and diastolic left ventricular function
Abstract
Background: Obesity is associated with increased cardiovascular morbidity and mortality. A direct effect of isolated obesity on cardiac function is not well established.
Objective: To determine the direct effect of different grades of isolated obesity on echocardiographic indices of systolic and diastolic left ventricular function.
Methods: 48 obese and 25 normal weight women were studied. They had no other pathological conditions. Obesity was classed as slight (n = 17; body mass index (BMI) 25-29.9 kg/m2), moderate (n = 20; BMI 30-34.9 kg/m2), or severe (n = 11; BMI > or = 35 kg/m2). Echocardiographic indices of systolic and diastolic function were obtained, and dysfunction was assumed when at least two values differed by > or = 2 SD from the normal weight group.
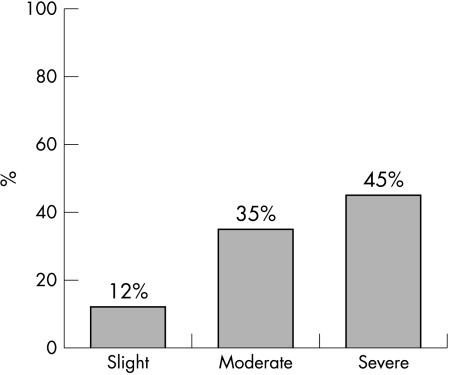
Results: Ejection fraction (p < 0.05), fractional shortening (p < 0.05), and mean velocity of circumferential shortening (p < 0.05) were increased in slight and moderate obesity. Left ventricular dimensions were increased (p < 0.001) but relative wall thickness was unchanged. No obese patients met criteria for systolic dysfunction. In obese subjects, the mitral valve pressure half time (p < 0.01) and the left atrial diameter (p < 0.001) were increased and the deceleration slope was decreased (p < 0.01); all other diastolic variables were unchanged. No differences were found between obesity subgroups. Subclinical diastolic dysfunction was more prevalent among obese subjects (p = 0.002), being present in two with slight obesity (12%), seven with moderate obesity (35%), and five with severe obesity (45%). BMI correlated significantly with indices of left ventricular function.
Conclusions: Subclinical left ventricular diastolic dysfunction is present in all grades of isolated obesity, correlates with BMI, and is associated with increased systolic function in the early stages of obesity.
Figures
Comment in
-
Cardiac function and obesity.Heart. 2003 Oct;89(10):1127-9. doi: 10.1136/heart.89.10.1127. Heart. 2003. PMID: 12975393 Free PMC article. No abstract available.
References
-
- Freedman DS, Williamson DF, Croft JB, et al. Relation of body fat distribution to ischemic heart disease. The National Health and Nutrition Examination survey I (NHANES I) epidemiologic follow-up study. Am J Epidemiol 1995;142:53–63. - PubMed
-
- Dwyer J. Policy and healthy weight. Am J Clin Nutr 1996;63(suppl):415–18. - PubMed
-
- Shaper AG. Obesity and cardiovascular disease. Ciba Found Symp 1996;201:90–107; 188–93. - PubMed
-
- Kannel WB, d’Agostino RB, Cobb J. Effect of weight on cardiovascular disease. Am J Clin Nutr 1996;63(suppl):419–22. - PubMed
-
- Jover Sanz E. Waist/hip ratio: obesity and cardiovascular risk. Ann Intern Med 1997;14:3–8. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous