

Management of fetal tachyarrhythmia based on superior vena cava/aorta Doppler flow recordings
- PMID: 12975422
- PMCID: PMC1767897
- DOI: 10.1136/heart.89.10.1211
Management of fetal tachyarrhythmia based on superior vena cava/aorta Doppler flow recordings
Abstract
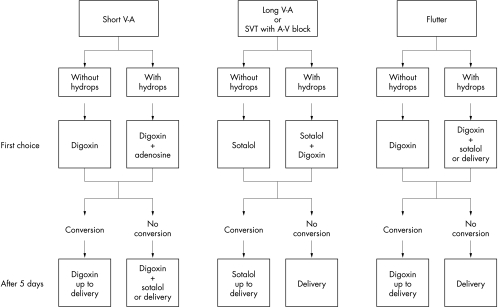
Objective: To evaluate a management protocol of fetal supraventricular tachycardia (SVT) based on prior identification of the underlying mechanism.
Design and setting: Prospective study in a mother-child tertiary university centre.
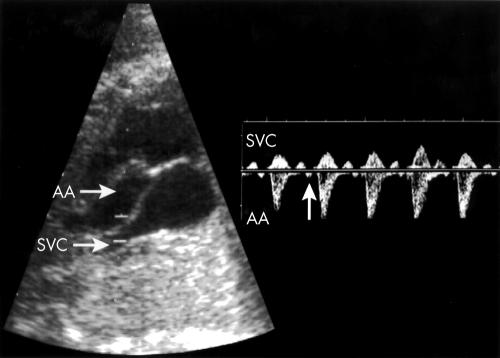
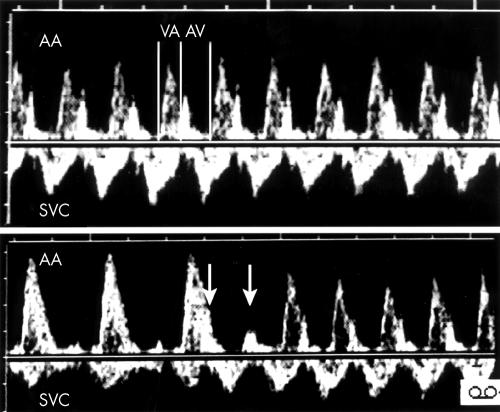
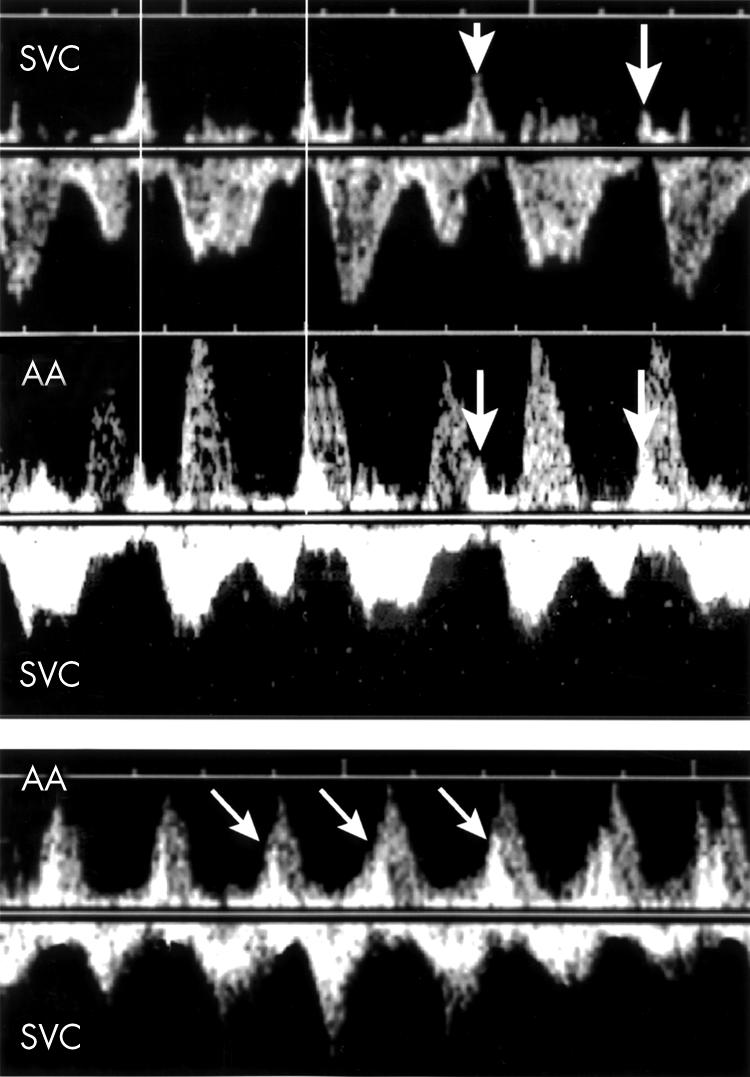
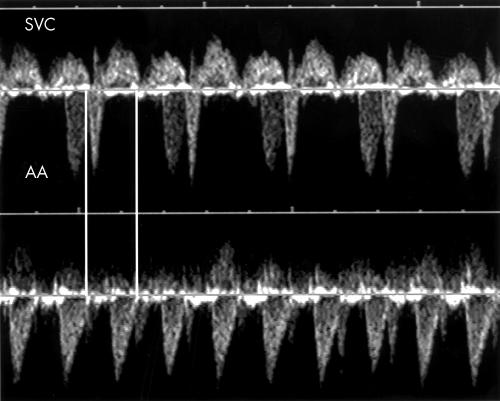
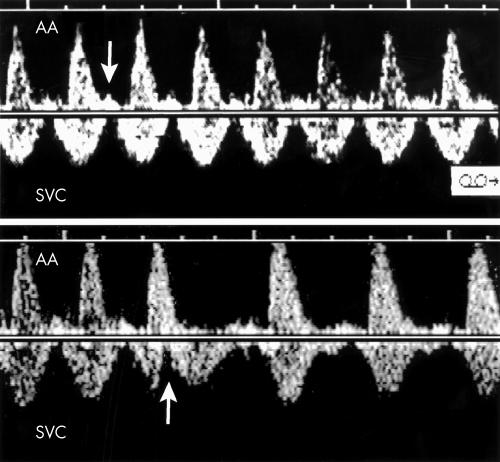
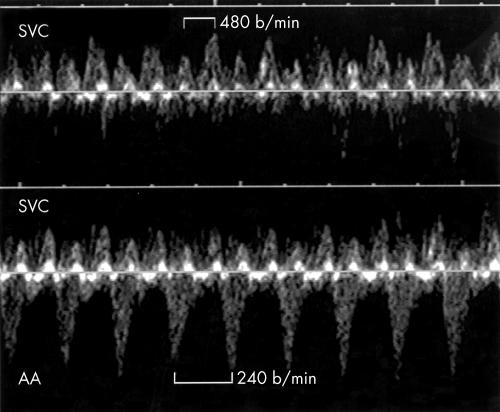
Patients: During a consecutive 36 month period, 18 fetuses with sustained SVT underwent a superior vena cava/ascending aorta (SVC/AA) Doppler investigation in an attempt to determine the atrioventricular (AV) relation and to treat the arrhythmia according to a pre-established management protocol.
Main outcome measure: Rate of conversion to sinus rhythm.
Results: Seven fetuses had short ventriculoatrial tachycardia, five of these with a 1:1 AV conduction suggesting re-entrant tachycardia. The first choice drug was digoxin and all were converted. One fetus had AV dissociation leading to the diagnosis of junctional ectopic tachycardia, which was resistant to digoxin and sotalol; amiodarone achieved postnatal conversion. One fetus had SVT and first or second AV block; the diagnosis was atrial ectopic tachycardia (AET), which responded to sotalol given as a drug of first choice. Seven fetuses had long ventriculoatrial tachycardia: one with sinus tachycardia (no treatment), one with permanent junctional reciprocating tachycardia (PJRT), and three with AET. The first choice drug was sotalol and all were converted. One AET was classified postnatally as PJRT. Six fetuses had intra-atrial re-entrant tachycardia: five with 2:1 AV conduction and one with variable block. The first choice drug was digoxin. Conversion was achieved in all but one, who died after birth from advanced cardiomyopathy.
Conclusion: The electrophysiological mechanisms of fetal SVT can be clarified with SVC/AA Doppler. The proposed management protocol has so far yielded a good rate of conversion to sinus rhythm.
Figures
References
-
- Benditt DG, Pritchett ELC, Smith WM, et al. Ventriculoatrial intervals: diagnostic use in paroxysmal supraventricular tachycardia. Ann Intern Med 1979;91:161–6. - PubMed
-
- Fouron JC, Proulx F, Miró J, et al. Doppler and M-mode ultrasonography to time fetal atrial and ventricular contractions. Obstet Gynecol 2000;96:732–6. - PubMed
-
- Erkkola R, Lammintausta R, Liukko P, et al. Transfer of propanolol and sotalol across the human placenta: their effect on maternal and fetal plasma renin activity. Acta Obstet Gynecol Scand 1982;61:31–4. - PubMed
-
- Houyel L, Fournier A, Ducharme G, et al. Electrophysiologic effects of sotalol on the immature mammalian heart. J Cardiovasc Pharmacol 1992;19:134–9. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical