

SMART: self-management of anticoagulation, a randomised trial [ISRCTN19313375]
- PMID: 13678426
- PMCID: PMC240084
- DOI: 10.1186/1471-2296-4-11
SMART: self-management of anticoagulation, a randomised trial [ISRCTN19313375]
Abstract
Background: Oral anticoagulation monitoring has traditionally taken place in secondary care because of the need for a laboratory blood test, the international normalised ratio (INR). The development of reliable near patient testing (NPT) systems for INR estimation has facilitated devolution of testing to primary care. Patient self-management is a logical progression from the primary care model. This study will be the first to randomise non-selected patients in primary care, to either self-management or standard care.
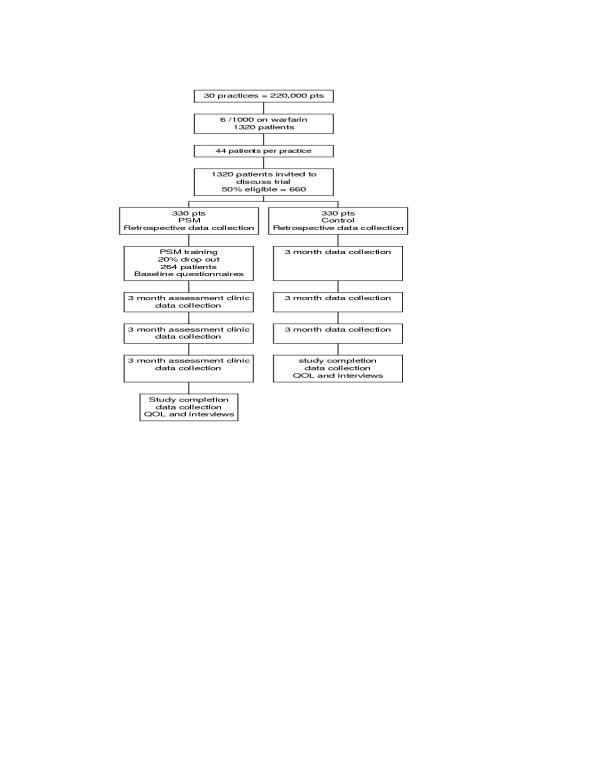
Method: The study was a multi-centred randomised controlled trial with patients from 49 general practices recruited. Those suitable for inclusion were aged 18 or over, with a long term indication for oral anticoagulation, who had taken warfarin for at least six months. Patients randomised to the intervention arm attended at least two training sessions which were practice-based, 1 week apart. Each patient was assessed on their capability to undertake self management. If considered capable, they were given a near patient INR testing monitor, test strips and quality control material for home testing. Patients managed their own anticoagulation for a period of 12 months and performed their INR test every 2 weeks. Control patients continued with their pre-study care either attending hospital or practice based anticoagulant clinics.
Discussion: The methodology used in this trial will overcome concerns from previous trials of selection bias and relevance to the UK health service. The study will give a clearer understanding of the benefits of self-management in terms of clinical and cost effectiveness and patient preference.
References
-
- Taylor F, Ramsay M, Covell B, Gaminara L, Thompson D, Cohen H, et al. Management of expanding anticoagulation clinics: a role for general practitioners. Br J Gen Pract. 1995;45:153–158.
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
