

Technical feasibility of embolizing aneurysms with glue (N-butyl 2-cyanoacrylate): experimental study in rabbits
- PMID: 13679265
- PMCID: PMC7973981
Technical feasibility of embolizing aneurysms with glue (N-butyl 2-cyanoacrylate): experimental study in rabbits
Abstract
Background and purpose: Liquid embolic agents may have potential as a therapeutic option to reconstruct a defective vessel wall. We evaluated the feasibility of transarterial glue embolization in surgically constructed carotid artery aneurysms.
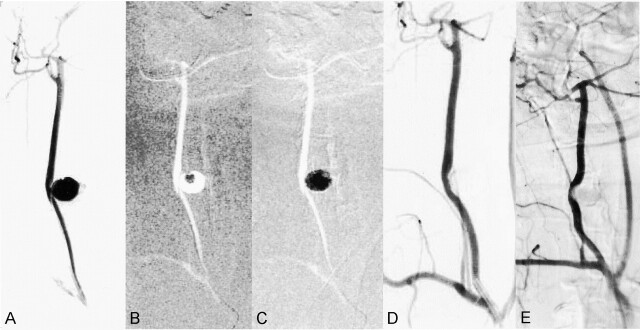
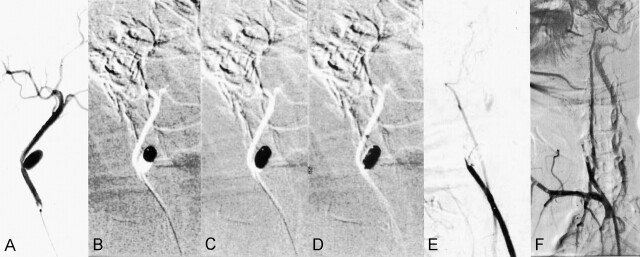
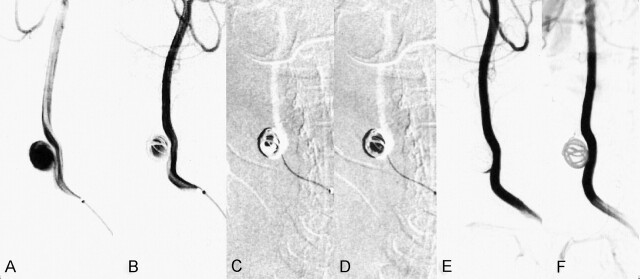
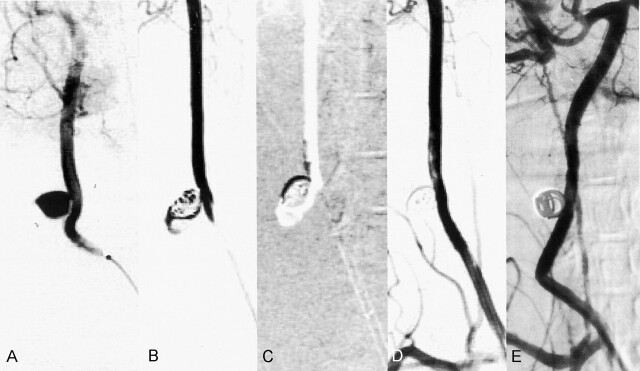
Methods: Reconstruction of arterial wall defects with use of glue casts was performed in 16 surgically constructed aneurysms of carotid arteries in rabbits. Via the transfemoral route, glue was injected without balloon protection through a microcatheter into the aneurysmal sac with (n = 8) and without (n = 8) a framework of coils. To identify safe and effective methods, four concentrations (28%, 33%, 40%, 50%) of glue-iodized oil mixtures were used in four aneurysms each. Immediate (n = 16) and 2-month follow-up (n = 10) postembolization angiograms were obtained to evaluate the residual aneurysmal sac and the carotid artery patency.
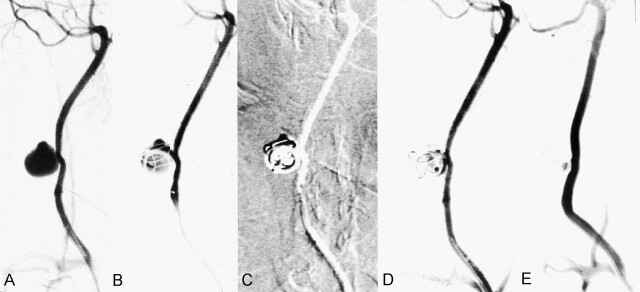
Results: Continuous column injection of glue was possible in all aneurysms, without fragmented migration of the injected glue cast. Catheter sticking or breakage did not occur during catheter retrieval. Glue embolization without a framework of coils (n = 8) resulted in complete obliteration of the aneurysmal sac in five aneurysms and incomplete obliteration with a small residual lumen in three. Two aneurysms resulted in carotid occlusion after catheter removal. A follow-up angiogram (n = 4) showed decreased residual lumen in two aneurysms, no change in the complete aneurysm occlusion in one, and carotid occlusion in one. Glue embolization with a coil framework (n = 8) resulted in complete obliteration of the aneurysmal sac in six aneurysms and incomplete obliteration with a small residual lumen in two. A small amount of spillage occurred in one owing to the improper position of the microcatheter caused by a difficult neck angle to the parent artery. Follow-up angiograms (n = 6) showed decreased residual lumen in one of two aneurysms and no change of the complete occlusion in five of six aneurysms.
Conclusion: Effective glue embolization into the aneurysmal sac is technically feasible. Microcatheter position within the aneurysm, concentration of glue, and direction of the aneurysmal neck angle all must be considered. With a coil framework, glue injection was more complete, without deformity or spillage of the glue from the aneurysm.
Figures
References
-
- Stehbens WE. Etiology of intracranial berry aneurysms. J Neurosurg 1989;70:823–831 - PubMed
-
- Mizutani T, Kojima H. Clinicopathological features of non-atherosclerotic cerebral arterial trunk aneurysms. Neuropathology 2000;1:91–97 - PubMed
-
- Guglielmi G, Vinuela F, Sepetka I, Macellari V. Electrothrombosis of saccular aneurysms via endovascular approach, I; electrochemical basis, technique, and experimental results. J Neurosurg 1991;75:1–7 - PubMed
-
- Viñuela F, Duckwiler G, Mawad M. Guglielmi detachable coil embolization of acute intracranial aneurysm: perioperative anatomical and clinical outcome in 403 patients. J Neurosurg 1997;86:475–482 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous