

Tacrolimus (FK 506)--a new therapeutic agent for severe recalcitrant psoriasis
- PMID: 1376102
- PMCID: PMC3208344
Tacrolimus (FK 506)--a new therapeutic agent for severe recalcitrant psoriasis
Abstract
Background: Psoriasis, a disease of unknown etiology, is in some patients severe, extremely debilitating, and unresponsive to conventional therapies, including UV-B, oral psoralen with long-wave UV radiation in the A range (PUVA), oral retinoids, and methotrexate. We report the results from our study of seven patients with refractory psoriasis who were treated with the new immunosuppressive drug, tacrolimus (FK 506).
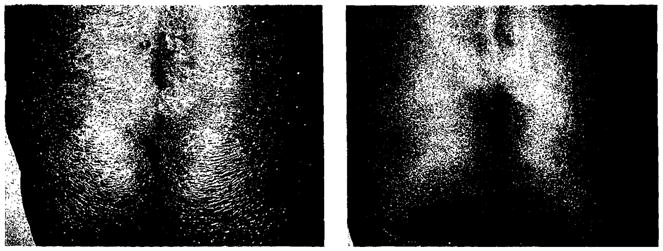
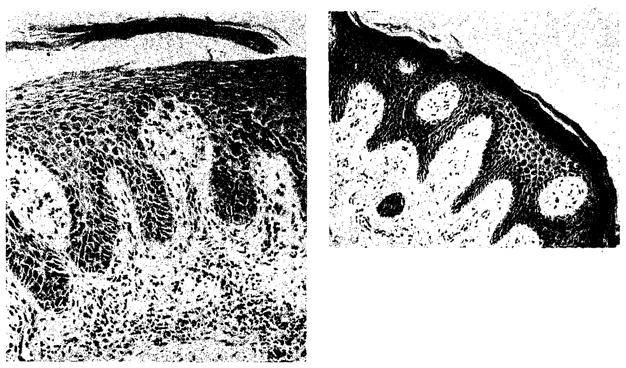
Observations: All seven patients showed a dramatic resolution of psoriasis that remained in remission as long as they received full-dose therapy. Serial skin biopsy specimens demonstrated a rapid disappearance of the inflammatory infiltrate and a slower resolution of the epidermal changes. Tacrolimus was well tolerated during the 5.5 to 14 months of observation. Side effects, including nephrotoxicity and hypertension, were controlled by appropriate modification of drug dosage.
Conclusions: Tacrolimus, a new immunosuppressive agent, is effective in treating patients with severe recalcitrant psoriasis. The mechanism of its action in psoriasis is unknown, but it may be related to its ability to modulate immune function. Further studies will establish criteria for patient selection and drug dosage, to maximize efficacy of this agent in psoriasis, while minimizing its toxicity.
Figures
References
-
- Krueger JG, Krane JF, Carter M, Gottlieb A. Role of growth factors, cytokines, and their receptors in the pathogenesis of psoriasis. J Invest Dermatol. 1990;94(suppl):1355–1405. - PubMed
-
- Basdsgaard O, Gupta A, Taylor S, Ellis C, Voorhees J, Cooper K. Psoriatic epidermal cells demonstrate increased numbers and function on non-Langerhans antigen presenting cells. J Invest Dermatol. 1989;92:190–195. - PubMed
-
- Müeller W, Hermann B. Cyclosporine A for psoriasis. N Engl J Med. 1979;301:555. - PubMed
-
- Ellis CN, Gorsulowsky DC, Hamilton T. Cyclosporine improves psoriasis in a double-blind study. JAMA. 1986;256:3110–3116. - PubMed
-
- Powles AV, Baker BS, Valdimarsson H, Holme B, Fry L. Four years of experience with cyclosporine A for psoriasis. Br J Dermatol. 1990;122 (suppl 36):13–19. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
