

EXTRACORPOREAL PERFUSION FOR OBTAINING POSTMORTEM HOMOGRAFTS
- PMID: 14087127
- PMCID: PMC3091281
Item in Clipboard
EXTRACORPOREAL PERFUSION FOR OBTAINING POSTMORTEM HOMOGRAFTS
Surgery.
1963 Dec.
No abstract available
Figures
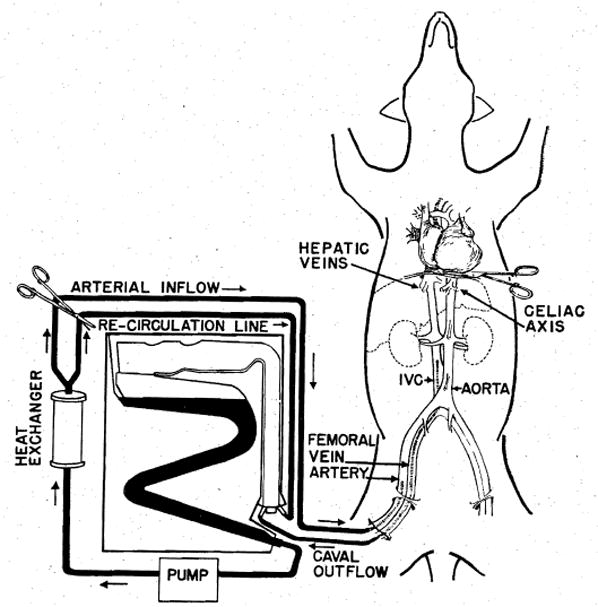
Technique of extracorporeal cadaver perfusion.
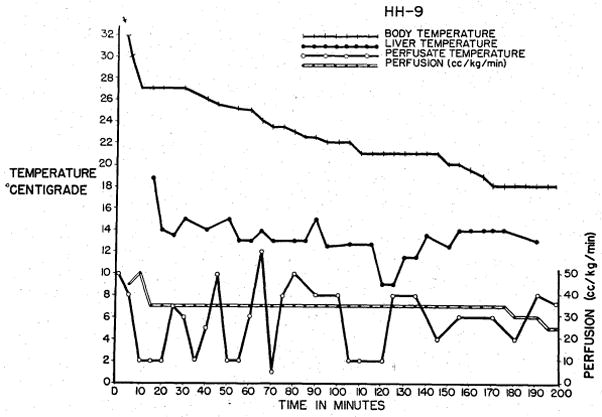
Cooling curves obtained during cadaver perfusion for a liver homograft. Note the rapid response of liver temperature to changes in perfusate temperature.
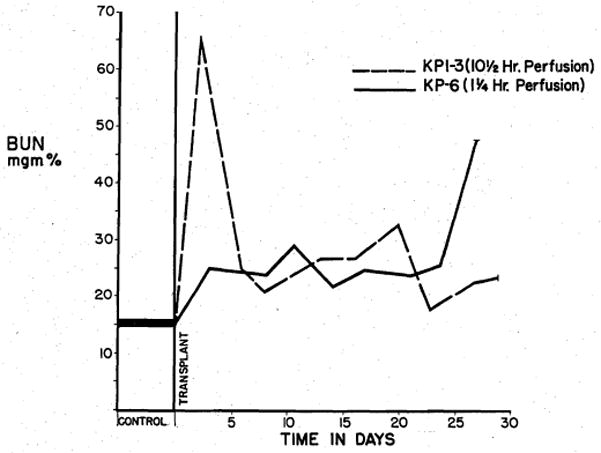
BUN level after renal homografting. Note the acute azotemia with the homograft perfused for 10½ hours. Early azotemia is minimal in the animal receiving a kidney perfused for 1¼ hours.
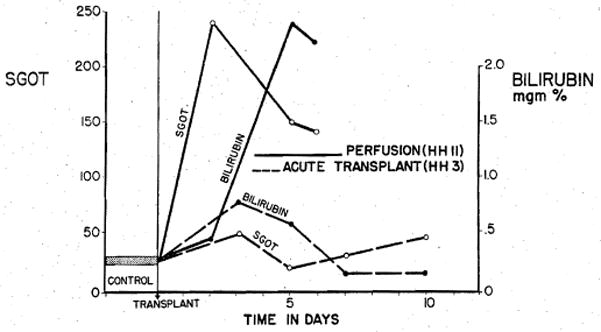
Patterns of injury in dogs observed following transplantation of a perfused hepatic homograft, and of a liver obtained after sacrifice of a living donor. Total time from death to reimplantation for the perfused organ was 140 minutes as compared to 55 minutes for the graft transplanted immediately after sacrifice (acute transplant).
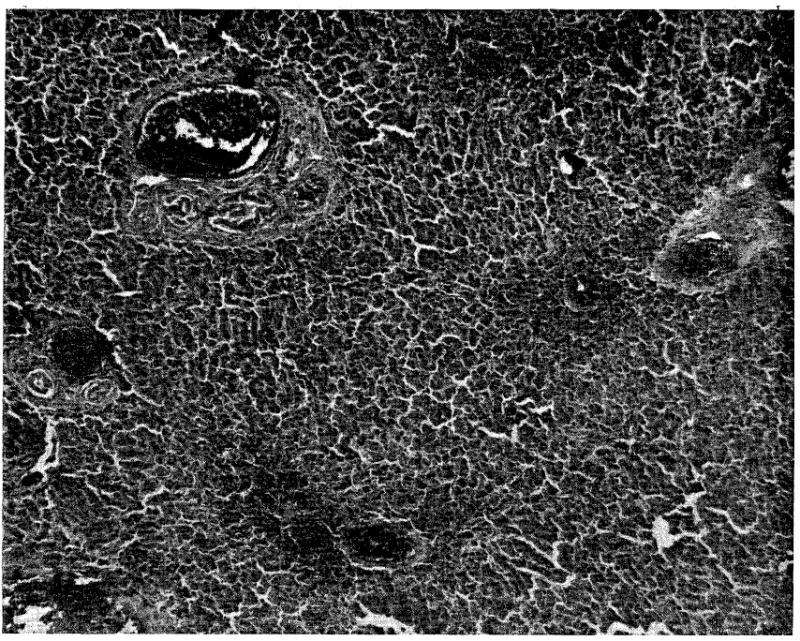
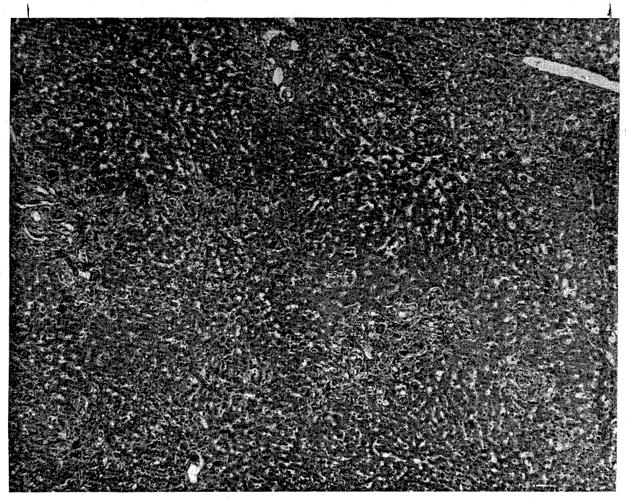
Typical injury observed in livers perfused for more than 2 hours. Note the marked centrilobular congestion and parenchymal necrosis. (×32.)
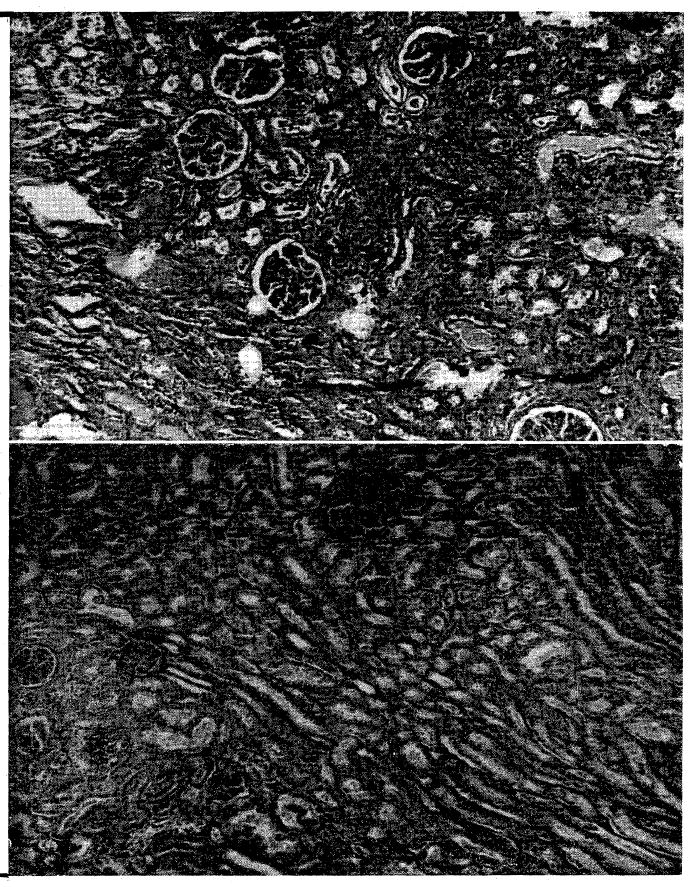
A, Appearance of homografted cadaveric left kidney 24 days after transplantation. B, Cadaveric contralateral kidney immediately after cessation of perfusion. (×32.)
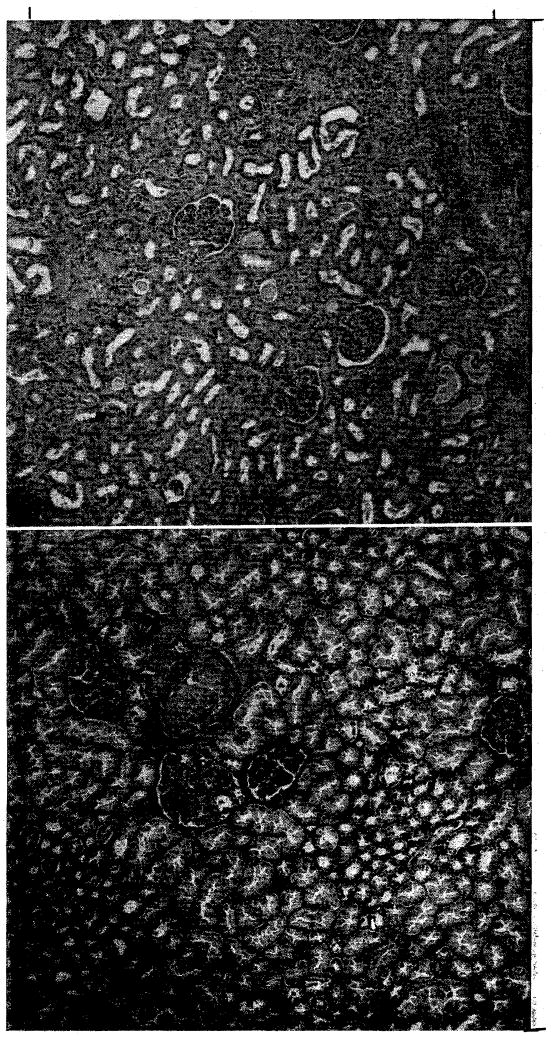
A, Homografted cadaveric right kidney removed 12 days after transplantation. Note rejection. B, Contralateral donor kidney obtained at conclusion of perfusion. (×32.)
Photomicrograph of first clinical hepatic homograft. The patient died on the operating table. Note advanced hepatic cell necrosis. (×32.)
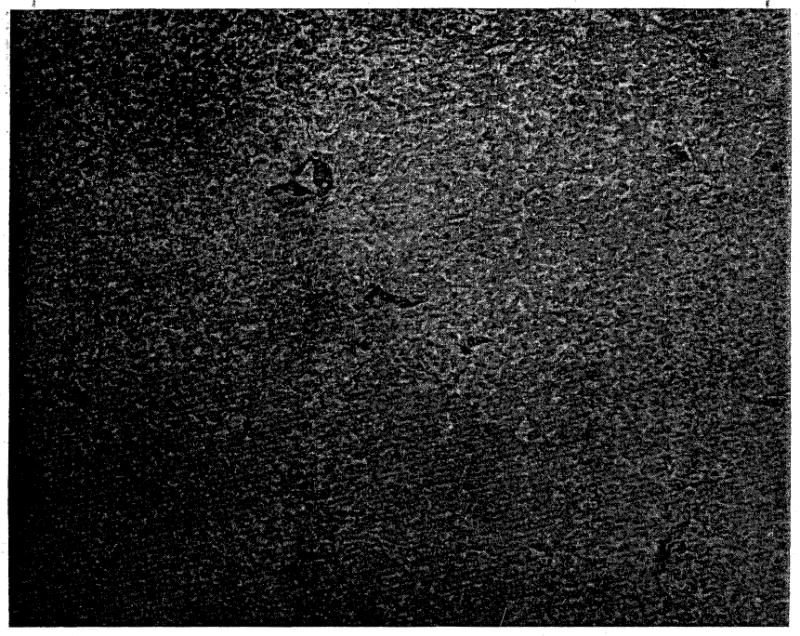
Photomicrograph of liver from the second clinical hepatic transplant, obtained at autopsy 22 days after transplantation. Note preservation of hepatic architecture. Moderate periportal fibrosis and bile stasis are present. (×32.)
References
-
- Blumenstock DA, Hechtman HB, Collins JA. Preservation of the canine lung. J Thoracic Surg. 1962;44:771. - PubMed
-
- Goodwin WE, Kaufman JJ, Mims MM, Turner RD, Glassock R, Goldman R, Maxwell MM. Human renal transplantation. I. Clinical experiences with 6 cases of renal transplantation. J Urol. 1963;89:13. - PubMed
-
- Huggins C, Carter E, McDermott W. Differential hypothermia in experimental hepatic surgery. A M A Arch Surg. 1957;74:327. - PubMed
-
- Humphries AL, Jr, Russell R, Ostofin J, Goodrich SM, Moretz WH. Successful reimplantation of dog kidney after 24 hour storage. S Forum. 1962;13:380. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous