

HOMOTRANSPLANTATION OF THE LIVER IN HUMANS
Surg Gynecol Obstet.
1963 Dec.
No abstract available
Figures
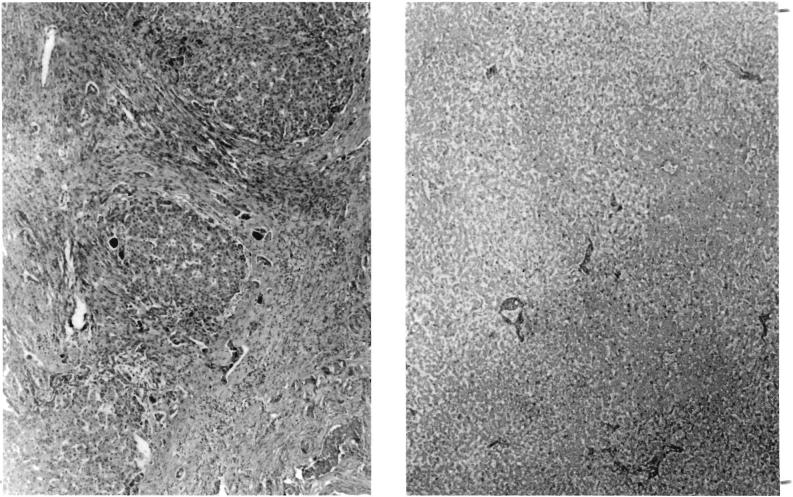
Liver tissue in Patient 1. A, left, Patient's own liver, showing advanced biliary cirrhosis. This 3 vear old child had congenital atresia of the bile ducts. B, right, Appearance of homotransplanted liver at autopsy, 12 hours after death. The patient exsanguinated on the operating table, 4 hours after revascularization of the homograft. Note extensive autolysis. Hematoxylin and eosin, X19.
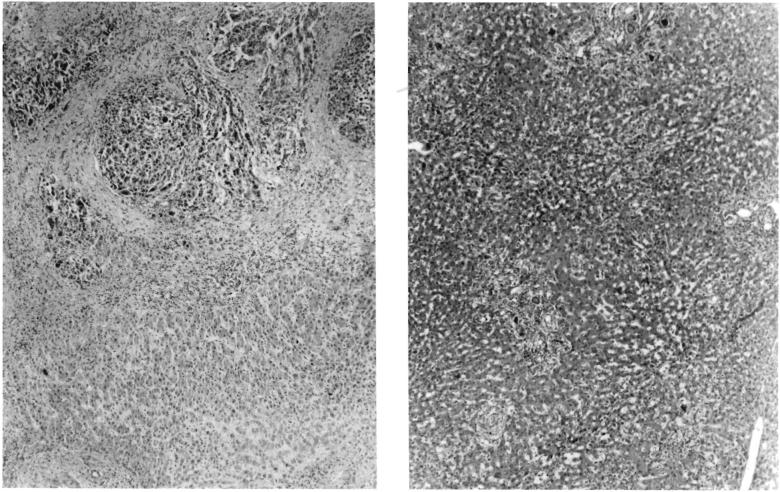
Specimens in Patient 2. A, left, Patient's own liver, showing hepatoma, B, right, Liver homograft obtained at autopsy 22 days after operation. Note good preservation of architecture. There was slight periportal fibrosis which is thought to have antedated transplantation. Note mild cholestasis and fatty metamorphosis. A few aggregates of mononuclear cells were present in the periportal areas. Hematoxylin and eosin, X19.
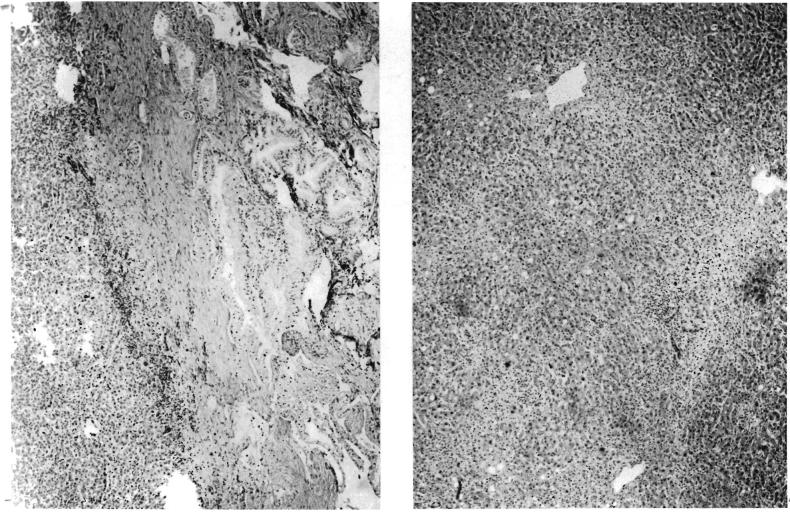
Specimens in Patient 3. A, left, Intrahepatic duct cell carcinoma which necessitated operation. B, right, Hepatic homograft 7½ days after transplantation. Note good state of preservation of parenchyma. Periportal accumulations of cells are principally neutrophiles. Hematoxylin and eosin, X19.
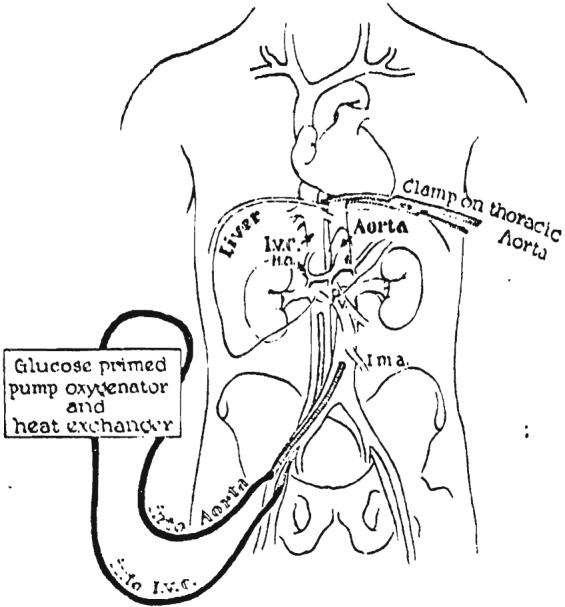
Extracorporcal perfusion of the cadaver donor. The venous drainage is from the inferior vena cava and the arterial inflow is through the aorta, both catheters being inserted through the femoral vessels. Note clamp on thoracic aorta to perfuse the lower half of the corpse selectively. A glucose primed pump oxygenator is used with a heat exchanger.
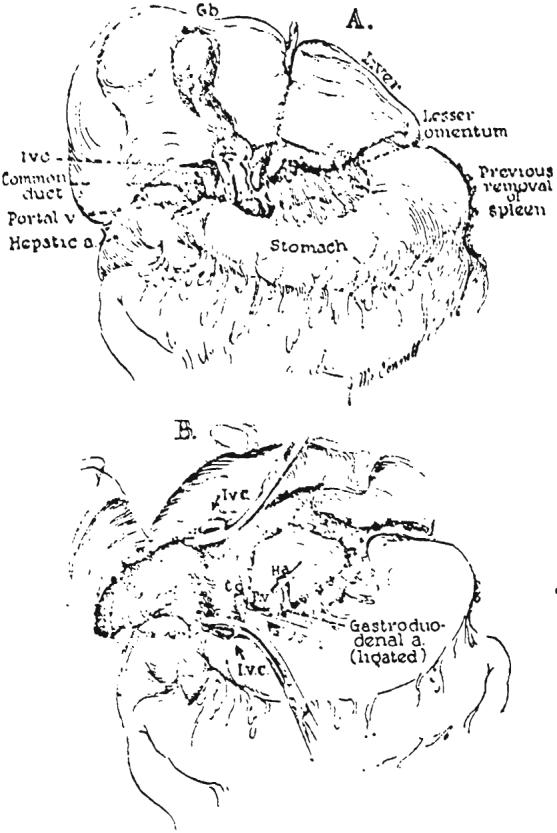
Final steps in removal of the liver. A, Dissection of the structures of the portal triad and division of the lesser omentum. B, Operative field after recipient hepatectomy.
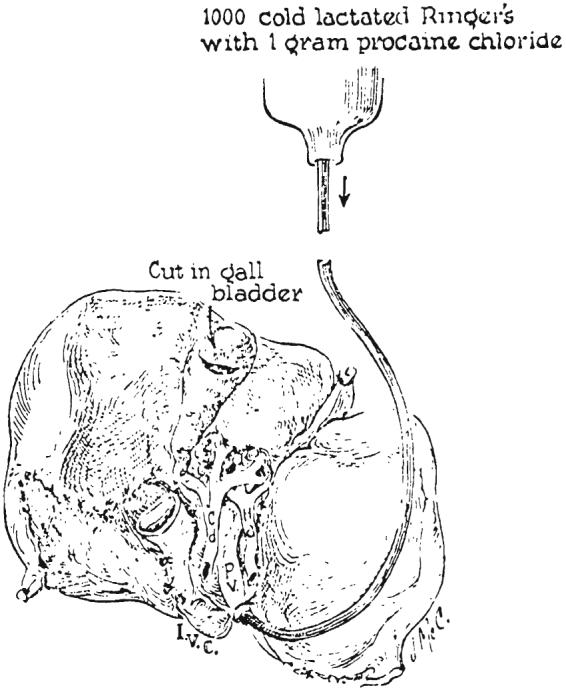
Donor liver after removal from cadaver. The blood is washed from the donor organ by gravity perfusion through the portal vein. Note the incision in the gallbladder, employed to prevent autolysis by entrapped bile during harvesting.
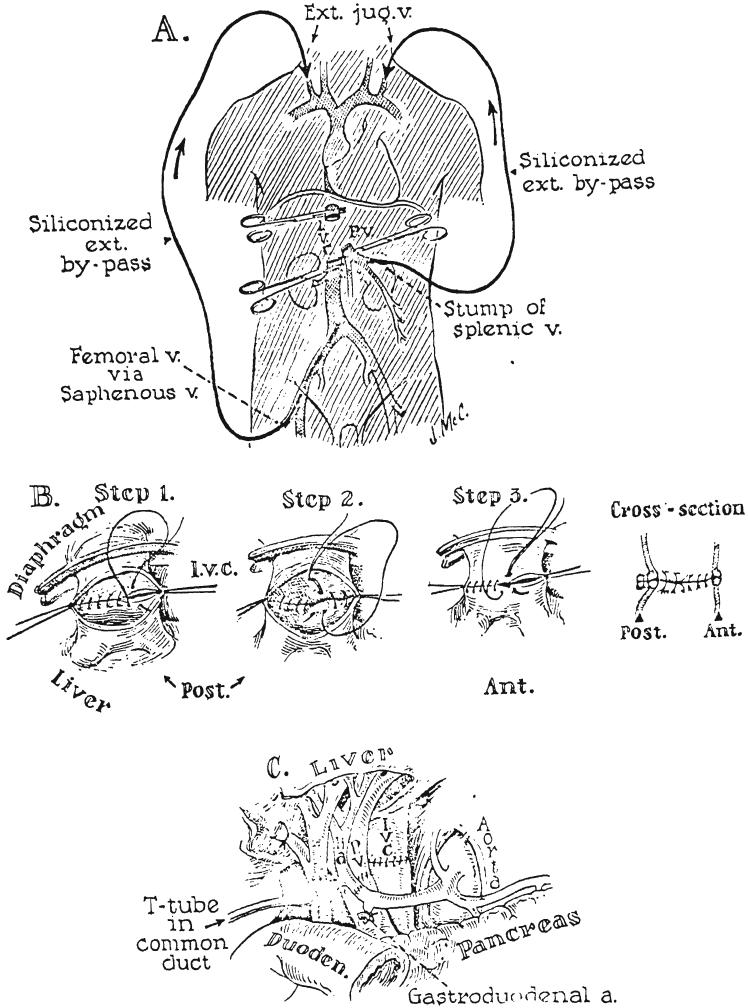
Anastomotic procedures in hepatic transplantation. A, External bypasses for decompression of the inferior vena caval and splanchnic venous beds. Both bypasses were inserted into the cervical jugular system. The splanchnic venous catheter used in Patient 2 was inserted after removal of the spleen. Portal decompression was found to be unnecessary providing the caval bypass functions satisfactorily and is of sufficiently large caliber. B, Anastomosis of suprahepatic inferior vena cava. Note that the cuff of the homograft is actually a confluence of the hepatic veins and the vena cava. The posterior row is performed in 2 everting layers. If considerations of time are not pressing, the anterior row is also doubly sutured. C, Subhepatic operative field at completion of all anastomoses. Note that gallbladder has been removed and that the T tube is inserted through a stab wound in the recipient portion of the composite common duct, with the upper limb passing through the anastomosis.
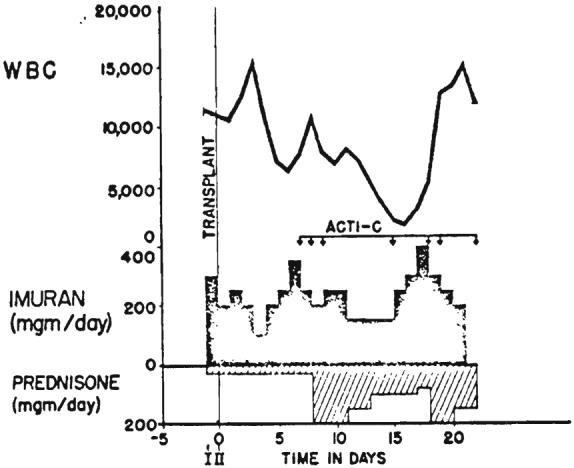
Pharmacologic therapy provided to prevent rejection in Patient 2. Avoidance of leukopenia was attempted by careful selection of doses of azathioprine (imuran). ACTI-C, Each arrow is 200 micrograms of intravenously administered actinomycin C. I, First stage operation; II, Second stage operation.

Thrombelastograms of Patient 1. A, B, Two hours after revascularization of homograft. Bleeding diathesis was evident clinically. Note onset of clot formation occurs at normal time, since “r” value—time from start of record to clot deposition—is normal. However, the clot is tiny and is lysed as fast as it is formed. C, D, Fifty and 20 per cent of normal fresh blood added to specimen A delays but does not prevent clot lysis. E, Recordings after 0.1 gram per kilogram intravenous EACA. Fibrinolytic activity is abolished. The abnormally small thrombelastogram is due to low fibrinogen. Hemostasis could never be obtained.
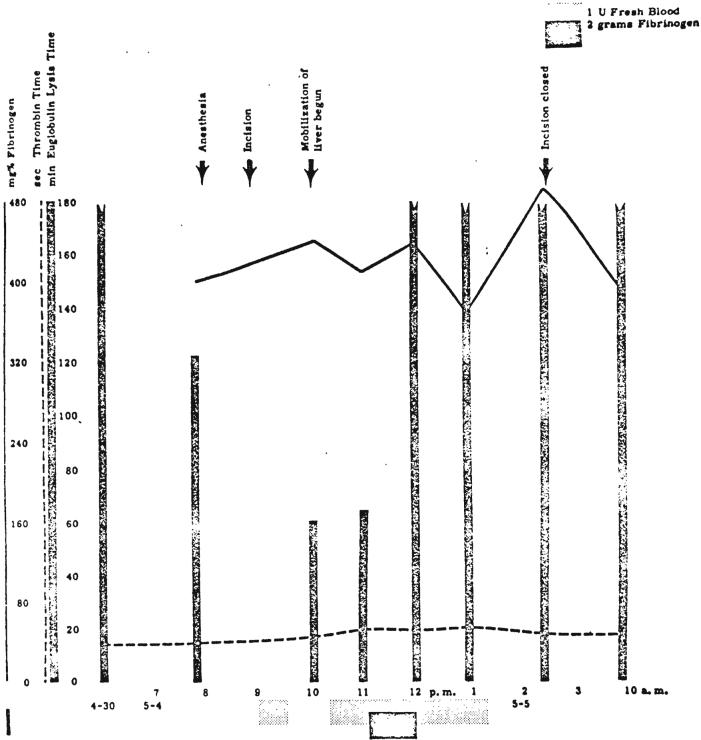
Changes in coagulation during first stage operation in Patient 2, when liver was prepared for subsequent removal. Note striking decrease in euglobulin lysis time during mobilization of liver.
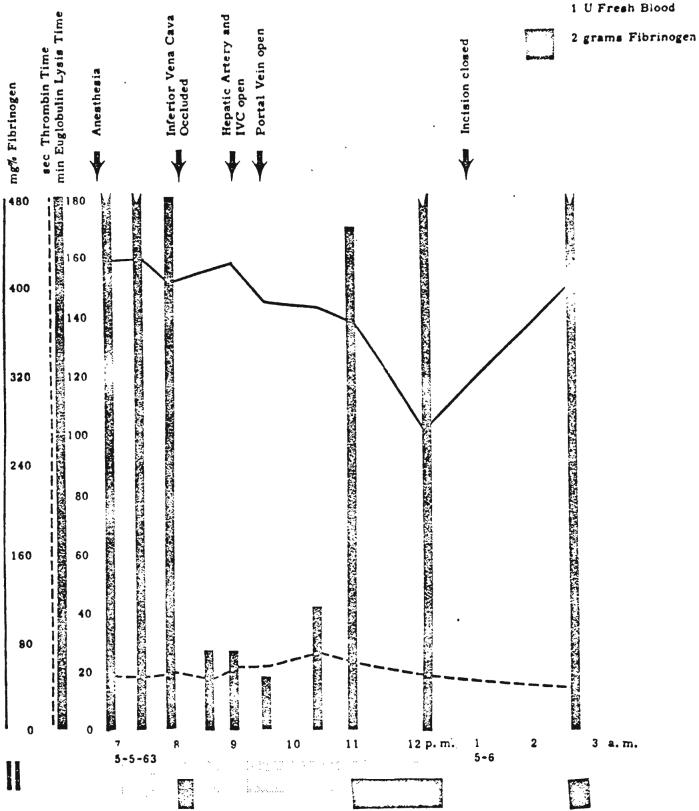
Changes in coagulation during definitive transplantation at second stage in Patient 2. Note drastic decrease in euglobulin lysis time and moderate delayed fall in fibrinogen level. EACA, 0.1 gram per kilogram, was given intravenously at 8:47 p.m.
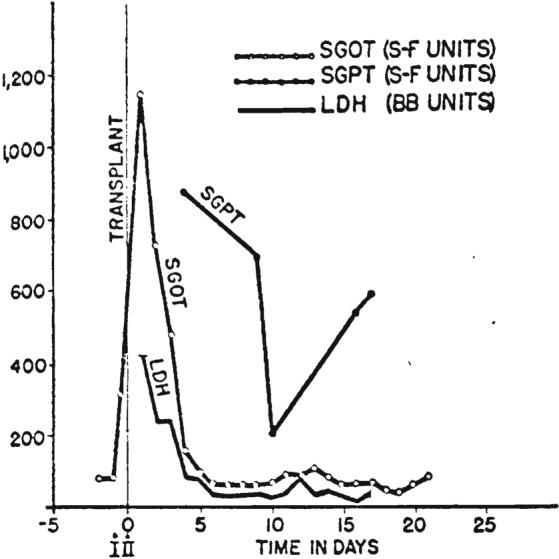
Graphic depiction of serum enzyme alterations following hepatic transplantation in Patient 2. Note immediate rise in SGOT with subsequent decline. LDH and SGPT were similarly affected.
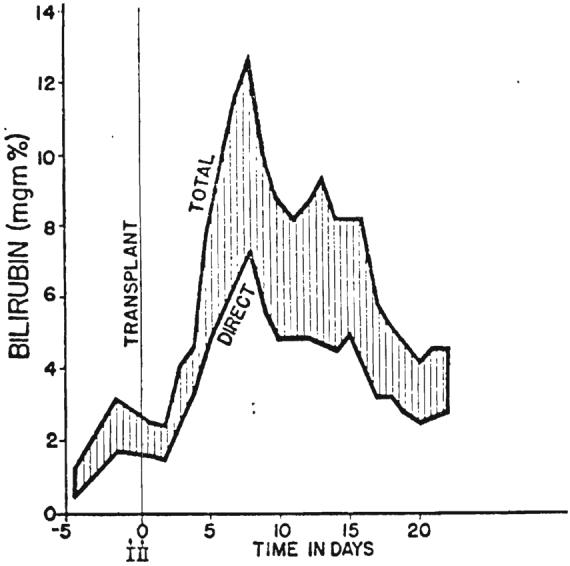
Graph showing rise in serum bilirubin to 12.8 milligrams per cent in Patient 2 nine days after transplantation. After transient deepening of jaundice there was progressive improvement.
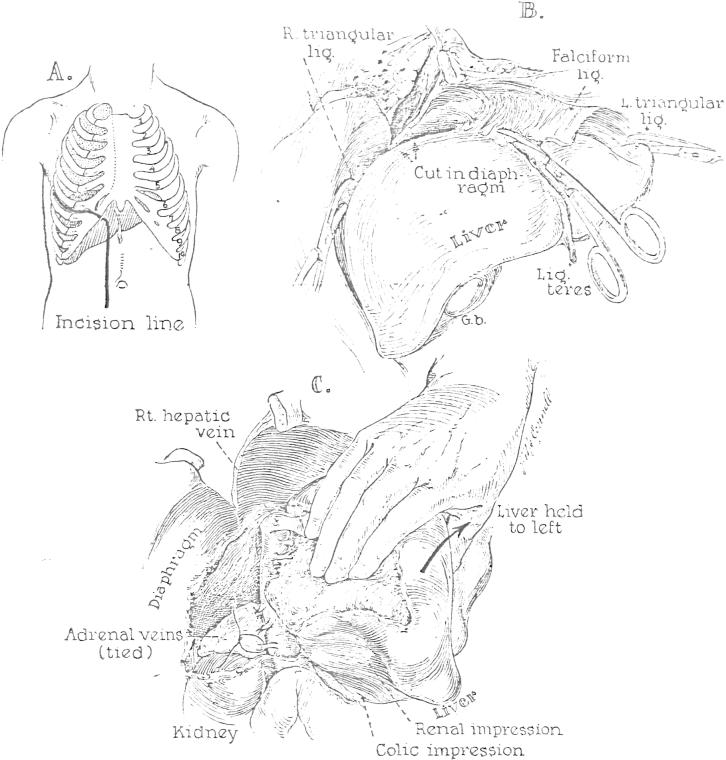
Preparation for extirpation of the liver. The steps followed are essentially the same for the donor and recipient operations. A, Line of incision used for all the cadavers and in Patient 2. B, Mobilization of the falciform, triangular, and coronary ligaments. C, Dissection of the right lateral and posterior surfaces of the inferior vena cava; ligation of the adrenal veins. After completion of this maneuver, it is possible to sweep the finger from the diaphragm to the renal veins without meeting resistance.
References
-
- CHILD CG. W. B. Saunders Co.; Philadelphia: 1954. The Hepatic Circulation and Portal Hypertension; p. 285.
-
- GOODRICH EO, WELCH HF, NELSON JA, BEECHER TS, WELCH CS. homotransplantation of the canine liver. Surgery. 1956;39:244. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources