

FACTORS IN SUCCESSFUL RENAL TRANSPLANTATION
Surgery.
1964 Jul.
No abstract available
Figures
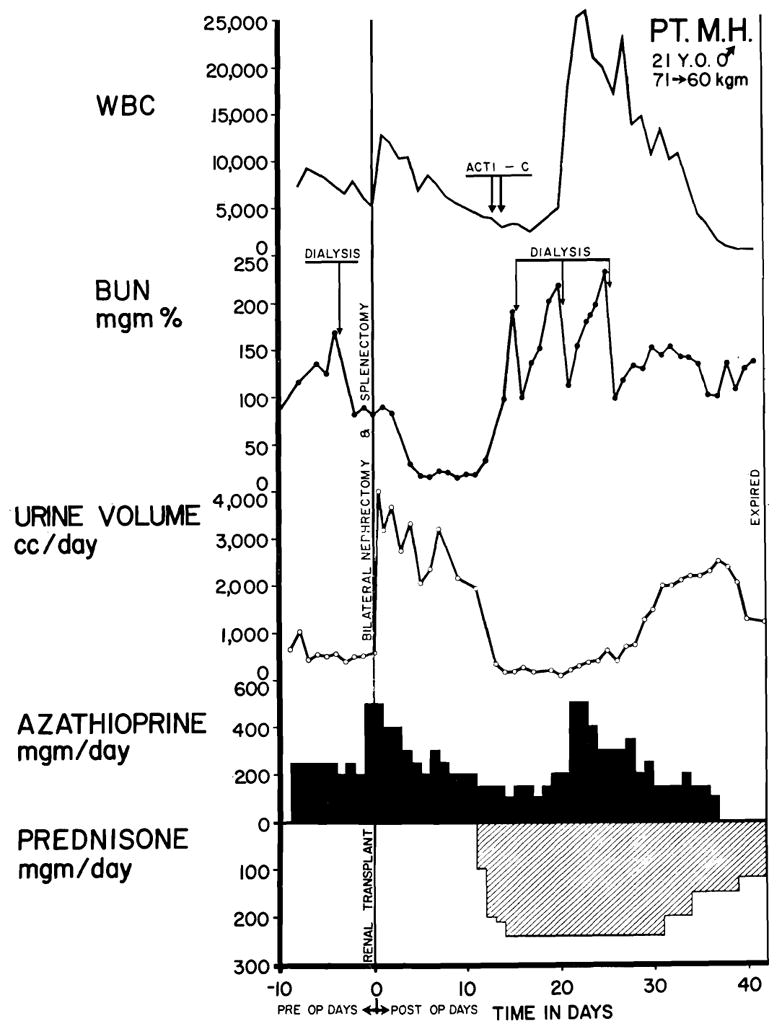
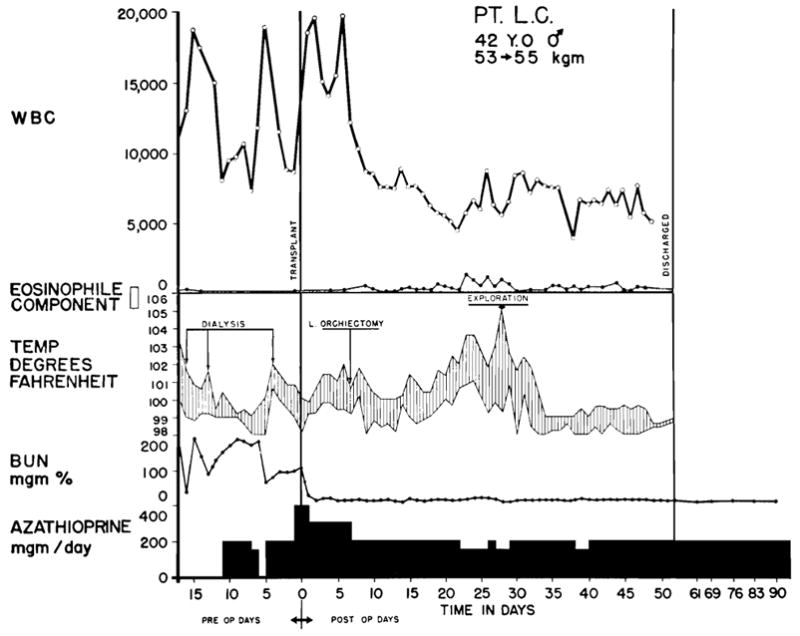
Typical case treated unsuccessfully. The kidney was obtained from the patient’s brother; both of them were of A+ blood type. Good renal function postoperatively was interrupted by a violent rejection crisis after 12 days and anuria developed. After 2 weeks of renal shutdown, secondary diuresis occurred. The patient died from drug toxicity, leukopenia, and septicemia (Table V, Case 32). Exceptionally vigorous rejection episodes seemed more common in recipients of blood type A than in those of other blood types. Note use of hemodialysis during height of rejection crisis. Acti C: each arrow represents the intravenous administration of 200 gamma actinomycin C.
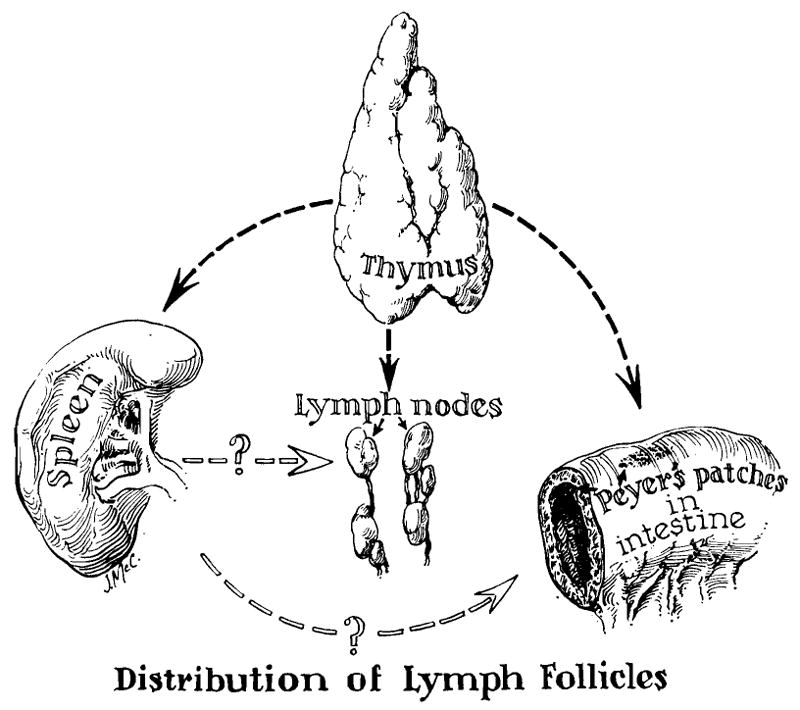
Theoretical considerations in the use of adjuvant thymectomy and splenectomy for the conditioning of recipient patients. The concept of the function of the thymus as an organizer in establishing fetal and neonatal immunologic reactivity is based largely on the work of Miller,, and may have no relevance in the adult animal. The role of the spleen in controlling response to antigenic stimuli in adult life is suggested by the work of Wissler and his colleagues., The contribution of these ancillary procedures to homograft survival is highly speculative at present.
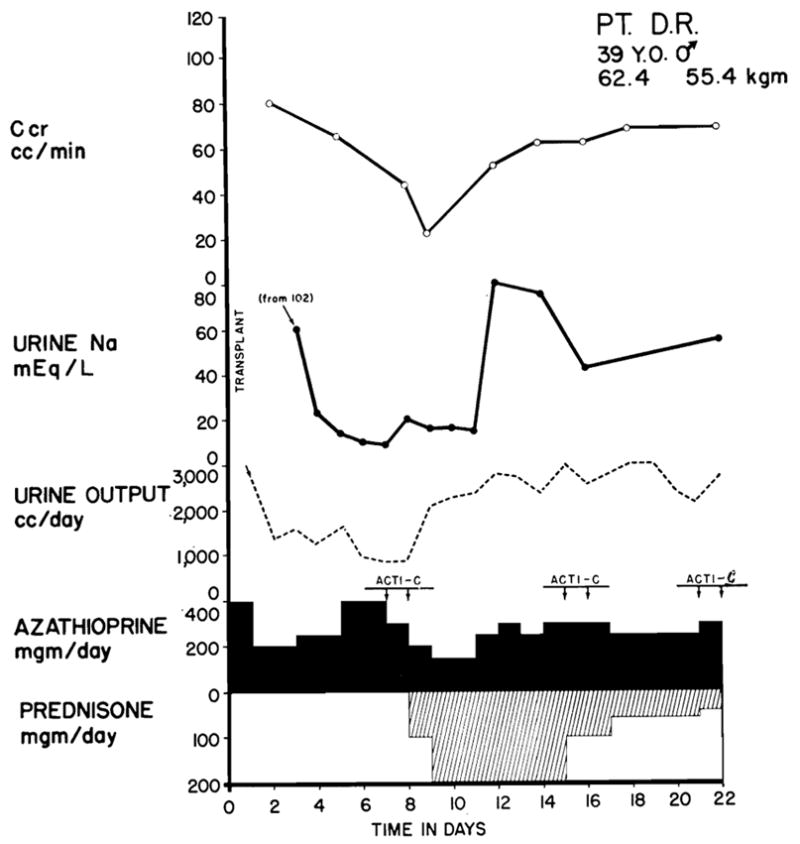
Typical case treated successfully. The patient received a kidney from his sister; both had type O blood. Fever, azotemia, hypertension, transplant wound tenderness, and proteinuria accompanied the relative oliguria and the decline in creatinine clearance which are depicted graphically. The changes were all reversed with the addition of prednisone and actinomycin C to the regimen. Leukopenia did not develop. Note the diminution of urine sodium concentration which is almost always observed during rejection and the paradoxical effect of prednisone in restoration of sodium excretion. Bilateral nephrectomy and splenectomy were performed at the same time as transplantation. Acti C: each arrow represents 200 gamma actinomycin C given intravenously.
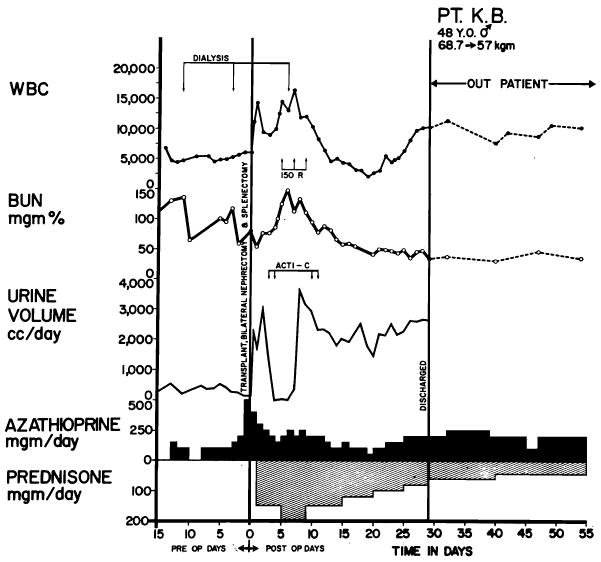
Value of Hume’s method of local irradiation in the treatment of severe rejection. The patient (A blood type) received a kidney from his sister (O blood type). After good initial function, gross hematuria developed, followed by anuria and other features of acute rejection. Wound tenderness, which was so extreme that urinary extravasation was feared, was largely relieved within an hour after the first dose of 150 r and resumption of urine excretion followed within 24 hours. The subsequent course was uncomplicated. Despite the rapidity of onset of rejection, it was possible, with 4 hourly analyses of urine composition, to demonstrate the changes that are thought to illustrate an ischemic component of rejection (see text and Fig. 3). Acti C: each arrow represents 200 gamma actinomycin C given intravenously. The conditions of x-ray therapy are described in the text.
Course of recovery in patient who did not have a classical rejection crisis. Evidence of an immunologic reaction was present after the second postoperative week with eosinophilia and high fever—findings which ultimately resolved spontaneously. The kidney for homograft was provided by his brother, both donor and recipient being A– blood type. The patient who was operated upon on July 5, 1963, continues to have normal renal function.
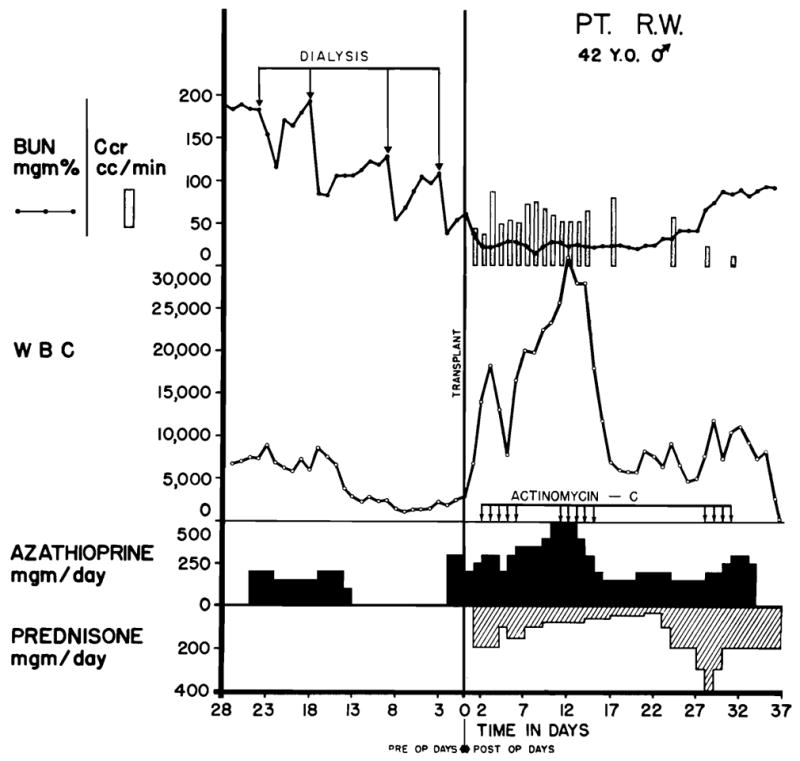
Fatal course of Case No. 24, a blood type A recipient. The donor was a convict volunteer of the same blood type. Note the precipitate drop in the white blood count in the last 2 days of life, a which time thrombocytopenia also developed. The cause of death was septicemia. Each arrow represents 200 gamma actinomycin C.
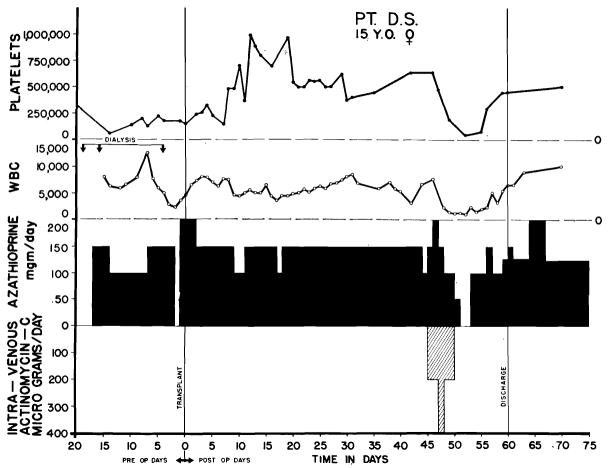
Demonstration of leukopenic and thrombocytopenic effect of actinomycin C. Note evidence of sudden bone marrow depression after 5 day course during which a total of 1,200 gamma was administered. After discontinuance of actinomycin C, it was possible to resume the previous dose schedule of azathioprine.
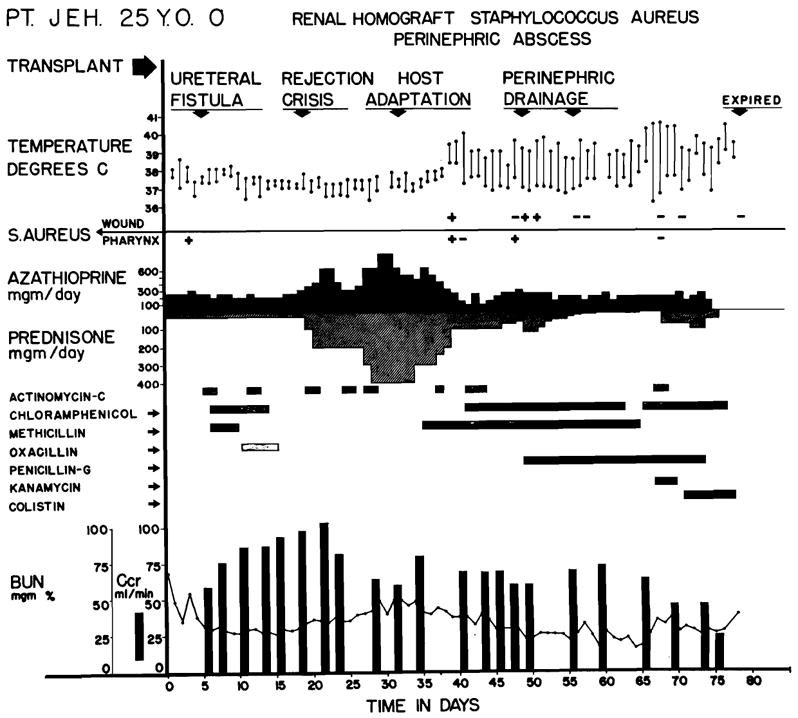
Course of Case No. 7. Fatal wound infection was first noted during late stages of the rejection crisis. Note that fever developed coincidentally with reversal of rejection and was uninfluenced by antibiotics or by surgical drainage. Death was due to septicemia. The simultaneous occurrence of rejection reversal and the development of uncontrollable sepsis suggested that loss of reactivity to bacterial and renal antigens may have occurred simultaneously.
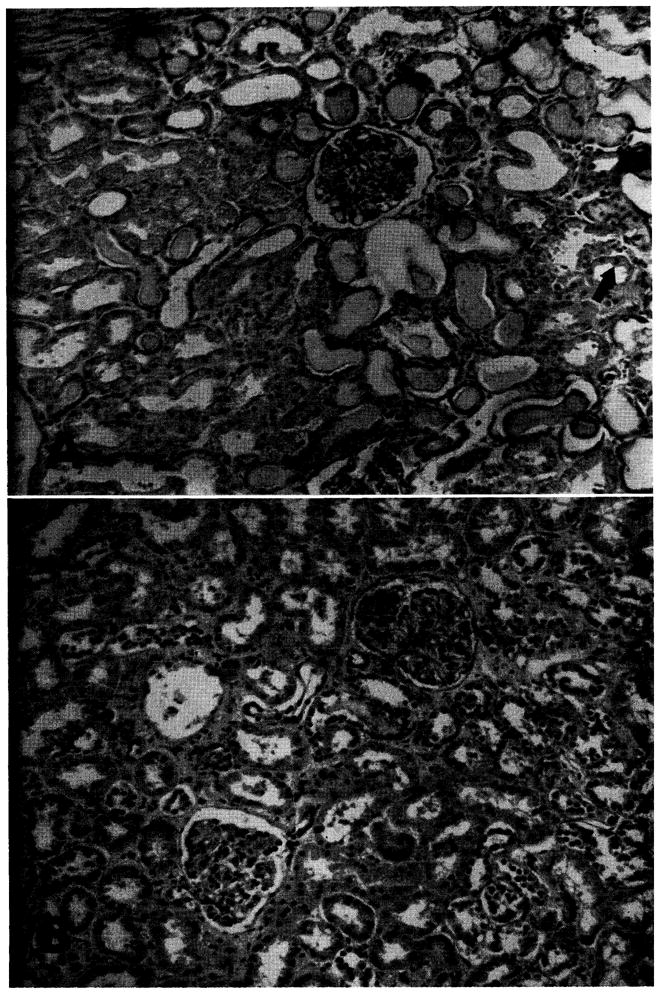
Homografts recovered at early and late autopsy. A, Case No. 29, 8 days after operation. Death was due to drug toxicity and septicemia that occurred after an early vigorous rejection with anuria. Note the evidence of acute tubular necrosis with necrotic and flattened tubular epithelium. Protein casts are evident. Mitosis is indicated by arrow. Cellular infiltrate is minimal. (Hematoxylin and eosin ×80; reduced ⅓.) Ba Case No. 38, 48 days after operation. A rejection episode had been successfully treated. Death was due to pneumonia. The kidney is essentially normal. (Hematoxylin and eosin ×80; reduced ⅓.)
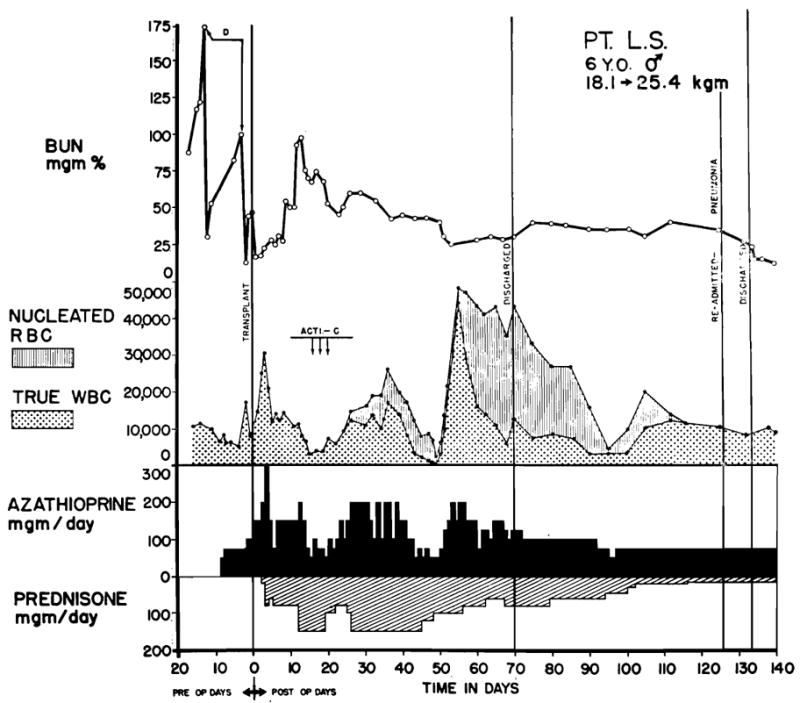
The appearance of nucleated red cells (normoblasts) in the peripheral blood after transplantation to a 6-year-old child. The child was O+ blood type. The maternal donor was A+. Note the high ratio of normoblasts to leukocytes. Drug dosages should be based upon the corrected rather than the falsely high peripheral count. Juvenile white cell forms are also frequently found at such times, although usually in smaller numbers. These changes are most marked in children, and are commonly associated with hyperpyrexia.
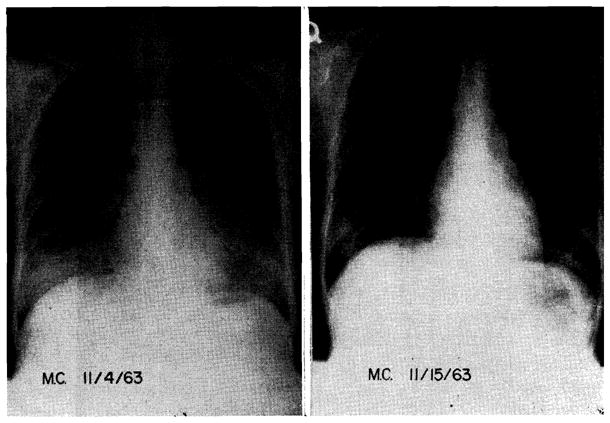
Diffuse bilateral pulmonary infiltrates in a 20-year-old girl of A+ blood type who received a kidney homograft from a convict donor of the same blood group. Note rapid resolution of the extensive infiltrations which first appeared 2 months after operation. Transplantation was performed on Sept. 3, 1963. After the near fatal pulmonary complication, the subsequent convalescence was without complication.
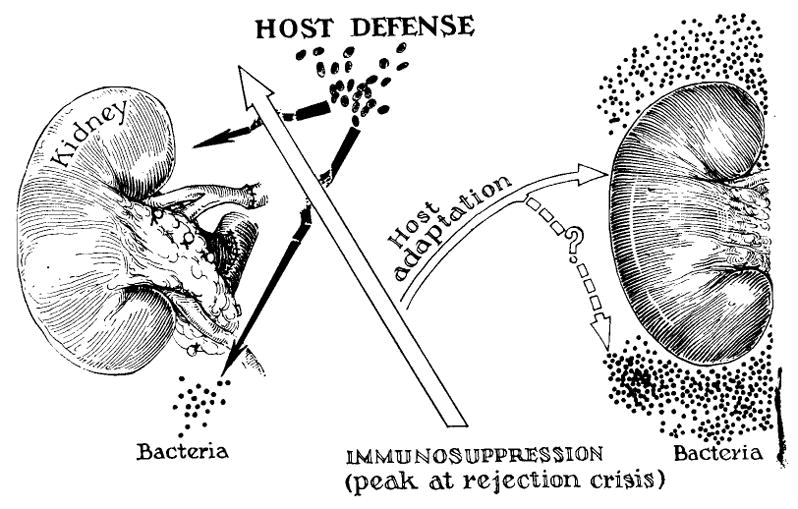
Possible mechanism of simultaneous loss of host reactivity to specific strains of endogenous bacteria, and to the alien renal tissue. See text.
References
-
- Bencosme SA, Lazarus SS. Pancreas of cortisone treated rabbits. A M A Arch Path. 1956;62:285. - PubMed
-
- Calne RY. Renal transplantation. Baltimore: Williams & Wilkins Company; 1963.
-
- Calne RY, Alexandre GPJ, Murray JE. A study of the effects of drugs in prolonging survival of homologous renal transplants in dogs. Ann New York Acad Sc. 1962;99:743. - PubMed
-
- Calne RY, Murray JE. Inhibition of the rejection of renal homografts in dogs by Burroughs Wellcome 57-322, S. Forum. 1961;12:118. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources