

Proactive asthma care in childhood: general practice based randomised controlled trial
- PMID: 14500440
- PMCID: PMC196449
- DOI: 10.1136/bmj.327.7416.659
Proactive asthma care in childhood: general practice based randomised controlled trial
Abstract
Objectives: To assess the feasibility and effectiveness of a general practice based, proactive system of asthma care in children.
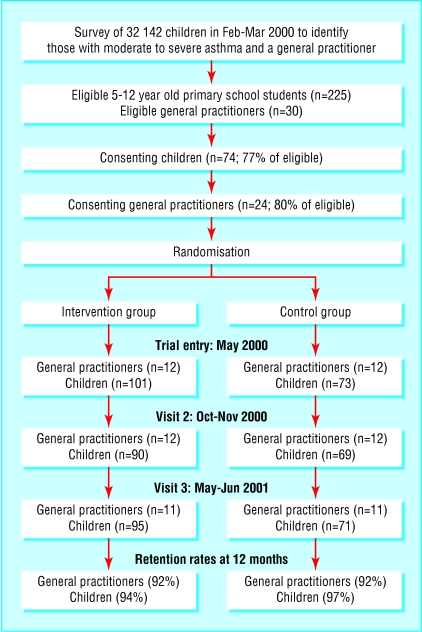
Design: Randomised controlled trial with cluster sampling by general practice.
Setting: General practices in the northern region of the Australian Capital Territory.
Participants: 174 children with moderate to severe asthma who attended 24 general practitioners.
Intervention: System of structured asthma care (the 3+ visit plan), with participating families reminded to attend the general practitioner.
Main outcome measures: Process measures: rates for asthma consultations with general practitioner, written asthma plans, completion of the 3+ visit plan; clinical measures: rates for emergency department visits for asthma, days absent from school, symptom-free days, symptoms over the past year, activity limitation over the past year, and asthma drug use over the past year; spirometric lung function measures before and after cold air challenge.
Results: Intervention group children had significantly more asthma related consultations (odds ratio for three or more asthma related consultations 3.8 (95% confidence interval 1.9 to 7.6; P = 0.0001), written asthma plans (2.2 (1.2 to 4.1); P = 0.01), and completed 3+ visit plans (24.2 (5.7 to 103.2); P = 0.0001) than control children and a mean reduction in measurements of forced expiratory volume in one second after cold air challenge of 2.6% (1.7 to 3.5); P = 0.0001) less than control children. The number needed to treat (benefit) for one additional written asthma action plan was 5 (3 to 41) children. Intervention group children had lower emergency department attendance rates for asthma (odds ratio 0.4 (0.2 to 1.04); P = 0.06) and less speech limiting wheeze (0.2 (0.1 to 0.4); P = 0.0001) than control children and were more likely to use a spacer (2.8 (1.6 to 4.7); P = 0.0001). No differences occurred in number of days absent from school or symptom-free day scores.
Conclusions: Proactive care with active recall for children with moderate to severe asthma is feasible in general practice and seems to be beneficial.
Figures
Comment in
-
Proactive asthma care does not suit everyone.BMJ. 2003 Nov 22;327(7425):1229. doi: 10.1136/bmj.327.7425.1229-b. BMJ. 2003. PMID: 14630780 Free PMC article. No abstract available.
References
-
- Wagner EH, Austin BT, von Korff M. Organizing care for patients with chronic illness. Milbank Q 1996;74: 511-44. - PubMed
-
- Gibson PG, Coughlan J, Wilson AJ, Abramson M, Bauman A, Hensley MJ, et al. Self-management education and regular practitioner review for adults with asthma. Cochrane Database Syst Rev 2003;(1): CD001117. - PubMed
-
- The International Study of Asthma and Allergies in Childhood (ISAAC) Steering Committee. Worldwide variation in prevalence of symptoms of asthma, allergic rhinoconjunctivitis, and atopic eczema: ISAAC. Lancet 1998;351: 1225-32. - PubMed
-
- National Asthma Council of Australia. Asthma management handbook 2002. www.nationalasthma.org.au/publications/amh/asthma_facts.htm (accessed 13 Mar 2003).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous