

Distal aortic perfusion and cerebrospinal fluid drainage for thoracoabdominal and descending thoracic aortic repair: ten years of organ protection
- PMID: 14501503
- PMCID: PMC1422700
- DOI: 10.1097/01.sla.0000086664.90571.7a
Distal aortic perfusion and cerebrospinal fluid drainage for thoracoabdominal and descending thoracic aortic repair: ten years of organ protection
Abstract
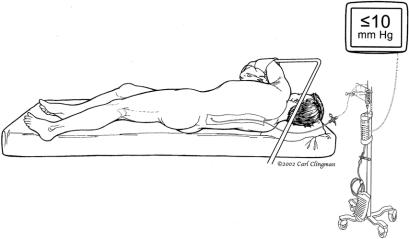
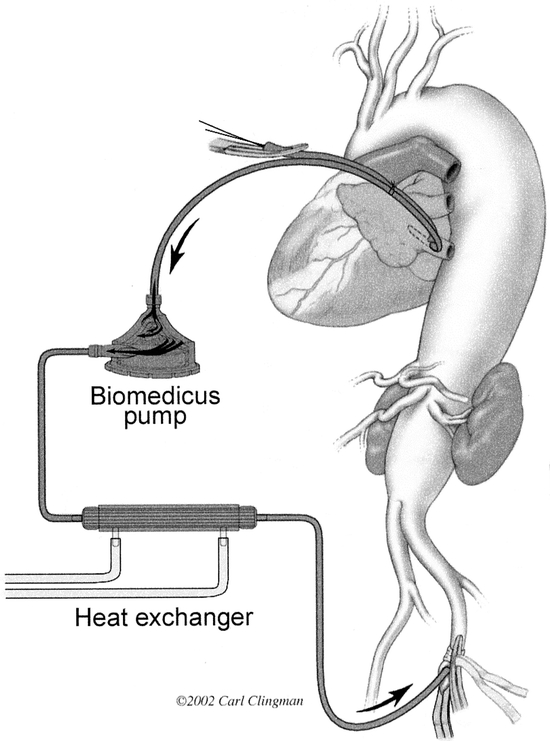
Objective: To report the long-term results of our experience using cerebrospinal fluid drainage and distal aortic perfusion in descending thoracic and thoracoabdominal aortic repair.
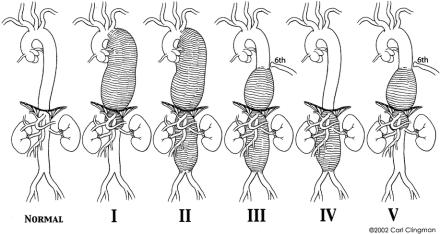
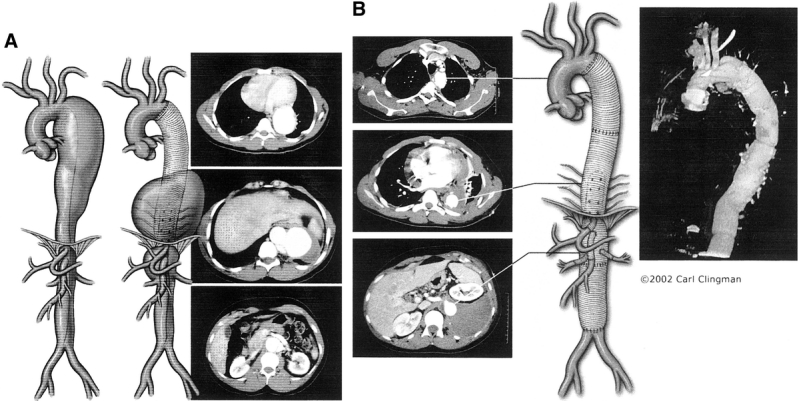
Summary background data: Repair of thoracoabdominal and thoracic aortic aneurysm by the traditional clamp-and-go technique results in a massive ischemic insult to several major organ systems. Ten years ago, we began to use distal aortic perfusion and cerebrospinal fluid drainage (adjunct) to reduce end-organ ischemia.
Methods: Between January 1991 and February 2003, we performed 1004 thoracoabdominal or descending thoracic repairs. Adjunct was used in 741 (74%) of 1004. Multivariable data were analyzed by Cox regression. Number needed to treat was calculated as the reciprocal of the risk difference.
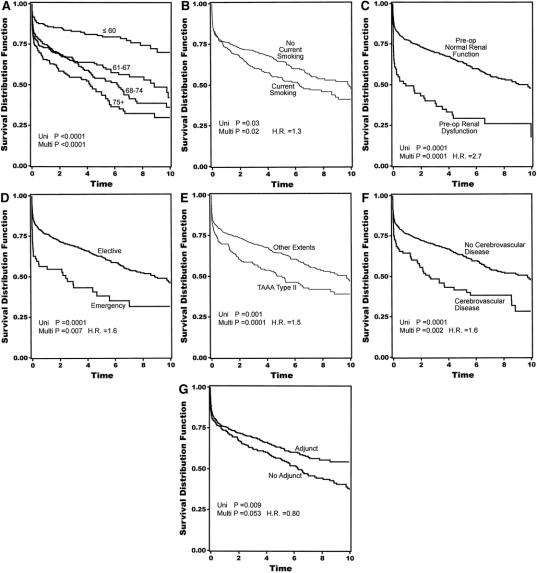
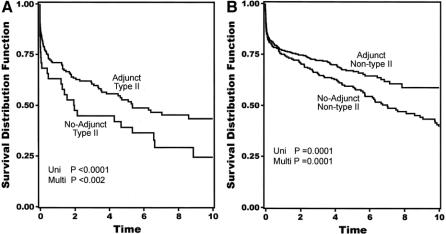
Results: Immediate neurologic deficit was 18 (2.4%) of 741 with adjunct and 18 (6.8%) of 263 without (P < 0.0009). In high-risk extent II aneurysms, the numbers were 11 (6.6%) of 167 with adjunct, and 11 (29%) of 38 without. Long-term survival was improved with adjunct (P < 0.002). The long-term survival results persisted after adjustment for age, extent II aneurysm, and preoperative renal function.
Conclusion: Use of adjunct over a long period of time has produced favorable results; approximately 1 neurologic deficit saved for every 20 uses of adjunct overall. In extent II aneurysms, where the effect is greatest, this increases to 1 saved per 5 uses. Adjunct is also associated with long-term survival, which is consistent with mitigation of ischemic end-organ injury. These long-term results indicate that cerebrospinal fluid drainage and distal aortic perfusion are safe and effective adjunct for reducing morbidity and mortality following thoracic and thoracoabdominal aortic repair.
Figures
References
-
- Crawford ES, Crawford JL, Safi HJ, et al. Thoracoabdominal aortic aneurysms: preoperative and intraoperative factors determining immediate and long-term results of operations in 605 patients. J Vasc Surg. 1986;3:389-404. - PubMed
-
- Cambria R, Davison J, Zannetti S, et al. Clinical experience with epidural cooling for spinal cord protection during thoracic and thoracoabdominal aneurysm repair. J Vasc Surg. 1997;25:241-243. - PubMed
-
- Coselli JS, LeMaire SA. Left heart bypass reduces paraplegia rates after thoracoabdominal aortic aneurysm repair. Ann Thorac Surg. 1999;67:1931-1934. - PubMed
-
- de Haan P, Kalkman CJ, Meylaerts SA, et al. Development of spinal cord ischemia after clamping of noncritical segmental arteries in the pig. Ann Thorac Surg. 1999;68:1278-1284. - PubMed
-
- Griepp RB, Ergin MA, Galla JD, et al. Minimizing spinal cord injury during repair of descending thoracic and thoracoabdominal aneurysms: the Mount Sinai approach. Semin Thorac Cardiovasc Surg. 1998;10:25-28. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
