

A national and single institutional experience in the contemporary treatment of acute lower extremity ischemia
- PMID: 14501504
- PMCID: PMC1422711
- DOI: 10.1097/01.sla.0000086663.49670.d1
A national and single institutional experience in the contemporary treatment of acute lower extremity ischemia
Abstract
Objective: To determine the contemporary clinical relevance of acute lower extremity ischemia and the factors associated with amputation and in-hospital mortality.
Summary background data: Acute lower extremity ischemia is considered limb- and life-threatening and usually requires therapy within 24 hours. The equivalency of thrombolytic therapy and surgery for the treatment of subacute limb ischemia up to 14 days duration is accepted fact. However, little information exists with regards to the long-term clinical course and therapeutic outcomes in these patients.
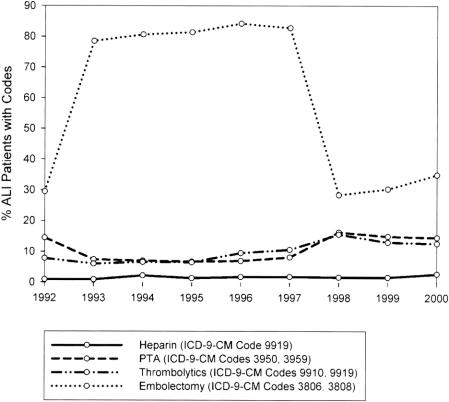
Methods: Two databases formed the basis for this study. The first was the National Inpatient Sample (NIS) from 1992 to 2000 of all patients (N = 23,268) with a primary discharge diagnosis of acute embolism and thrombosis of the lower extremities. The second was a retrospective University of Michigan experience from 1995 to 2002 of matched ICD-9-CM coded patients (N = 105). Demographic factors, atherosclerotic risk factors, the need for amputation, and in-hospital mortality were assessed by univariate and multivariate logistic regression analysis.
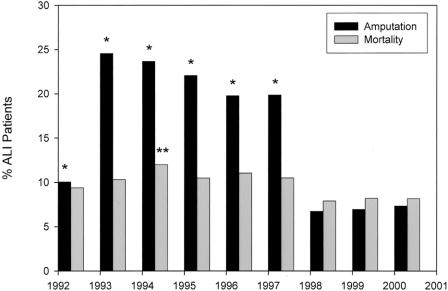
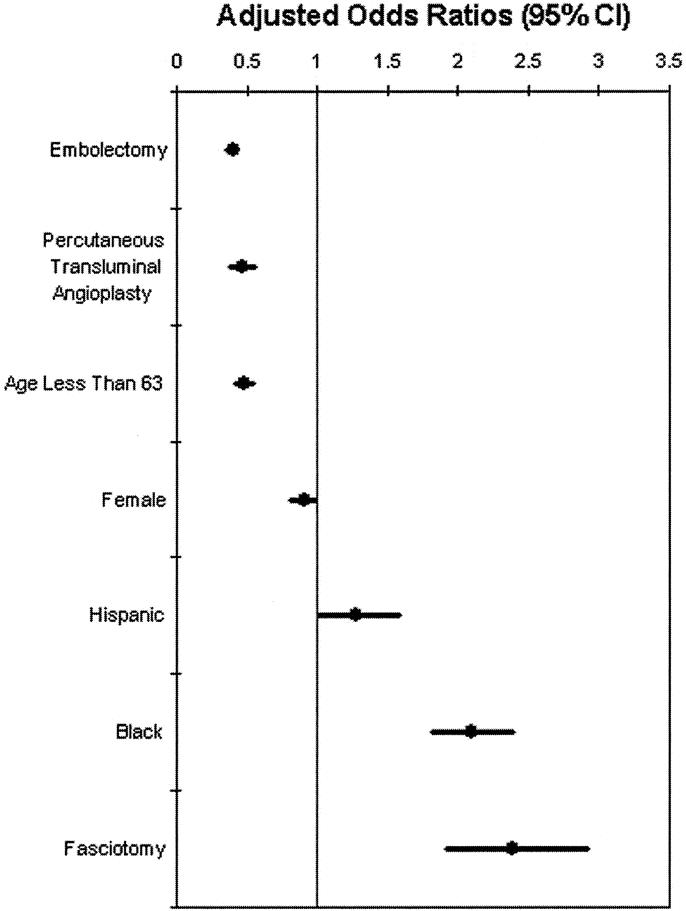
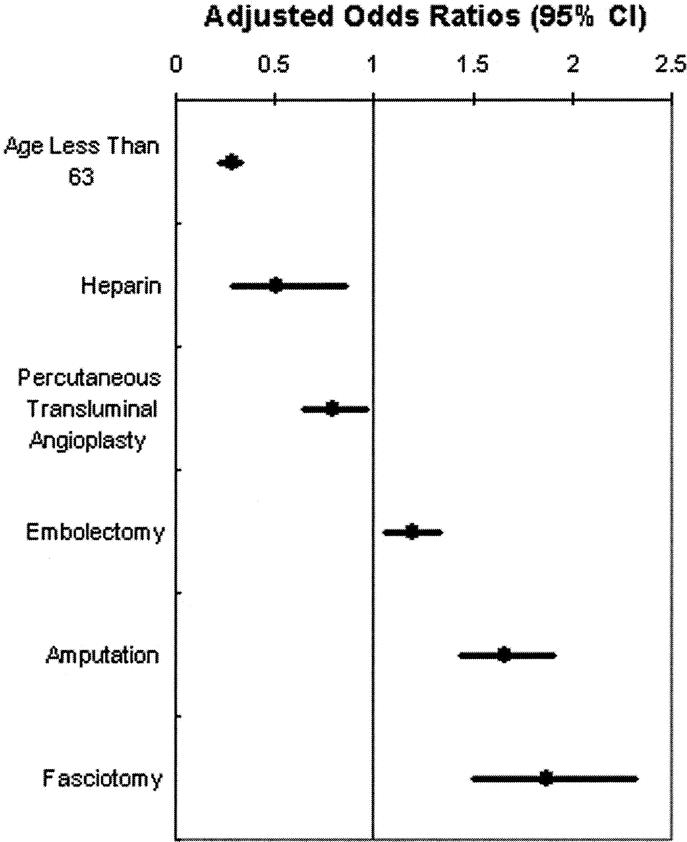
Results: In the NIS, the mean patient age was 71 years, and 54% were female. The average length of stay (LOS) was 9.4 days, and inflation-adjusted cost per admission was $25,916. The amputation rate was 12.7%, and mortality was 9%. Decreased amputation rates accompanied: female sex (0.90, 0.81-0.99), age less than 63 years (0.47, 0.41-0.54), angioplasty (0.46, 0.38-0.55), and embolectomy (0.39, 0.35-0.44). Decreased mortality accompanied: angioplasty (0.79, 0.64-0.96), heparin administration (0.50, 0.29-0.86), and age less than 63 years(0.27, 0.23-0.33). The University of Michigan patients' mean age was 62 years, and 57% were men. The LOS was 11 days, with a 14% amputation rate and a mortality of 12%. Prior vascular bypasses existed in 23% of patients, and heparin use was documented in 16%. Embolectomy was associated with decreased amputation rates (0.054, 0.01-0.27) and mortality (0.07, 0.01-0.57).
Conclusions: In patients with acute limb ischemia, the more widespread use of heparin anticoagulation and, in select patients, performance of embolectomy rather than pursuing thrombolysis may improve patient outcomes.
Figures
References
-
- National Hospital Discharge Survey Data. [database online]. Hyattsville, MD: National Center for Health Statistics; 2002. Updated November, 2002.
-
- Singh S, Evans L, Datta D, et al. The costs of managing lower limb-threatening ischaemia. Eur J Vasc Endovasc Surg. 1996;12:359-362. - PubMed
-
- Hoch JR, Tullis MJ, Acher CW, et al. Thrombolysis versus surgery as the initial management for native artery occlusion: efficacy, safety, and cost. Surgery. 1994;116:649-656. - PubMed
-
- Ouriel K, Shortell CK, De Weese JA, et al. A comparison of thrombolytic therapy with operative vascularization in the initial treatment of acute peripheral arterial ischemia. J Vasc Surg. 1994;19:1021-1030. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
