

Long-term functional results after ileal pouch anal restorative proctocolectomy for ulcerative colitis: a prospective observational study
- PMID: 14501509
- PMCID: PMC1422709
- DOI: 10.1097/01.sla.0000086658.60555.ea
Long-term functional results after ileal pouch anal restorative proctocolectomy for ulcerative colitis: a prospective observational study
Abstract
Objective: To document functional results in patients treated with an ileal pouch anal anastomosis (IPAA).
Summary background data: The restorative proctocolectomy with IPAA has become the procedure of choice for patients with ulcerative colitis, yet the long-term functional results are not well known.
Methods: We performed this prospective observational study in 391 consecutive patients (56% male; mean age, 33.7 +/- 10.8 years; range, 12-66 years) who underwent an IPAA between 1987 and 2002 (mean follow-up, 33.6 months; range, 0 to 180 months).
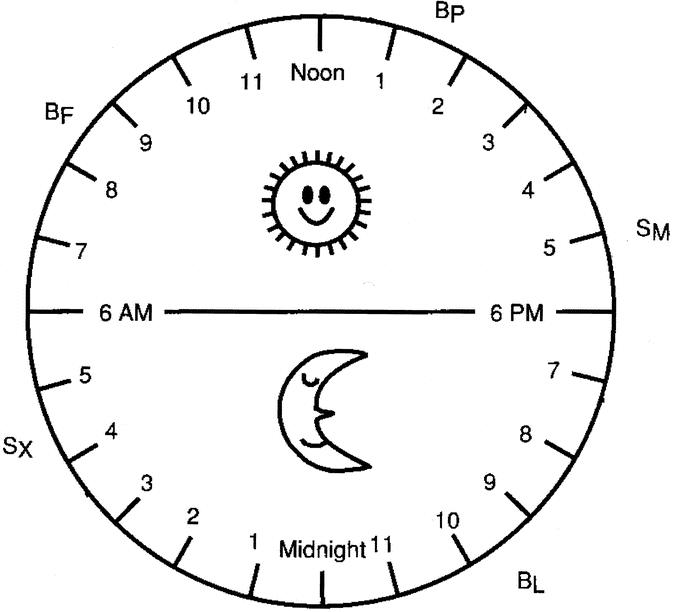
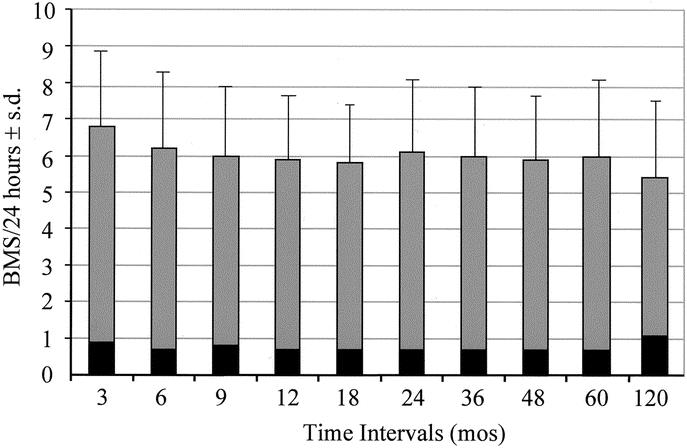
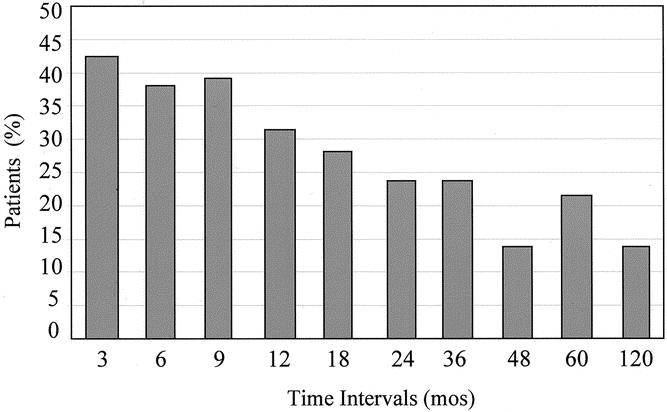
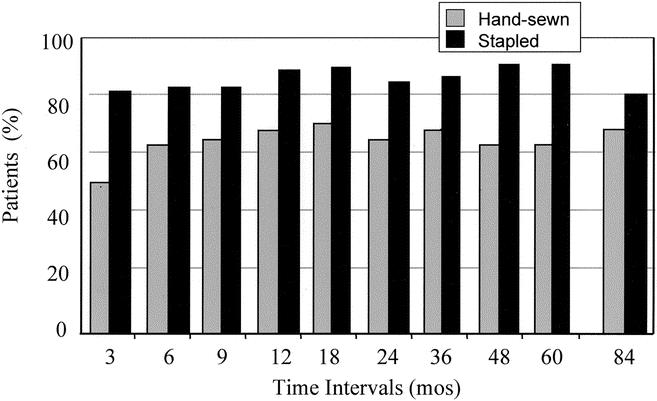
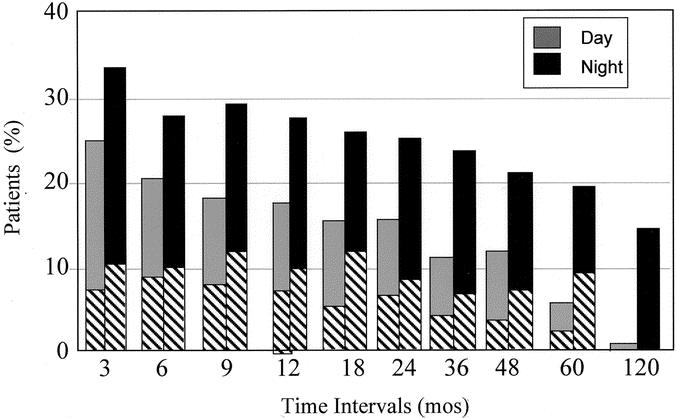
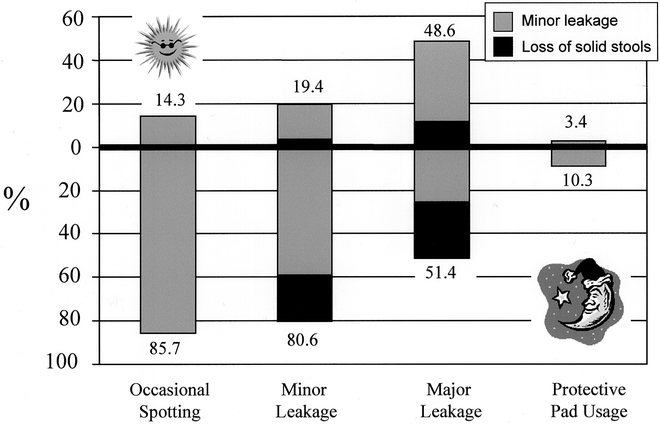
Results: The majority of patients underwent the procedure under elective circumstances with a hand-sewn ileal pouch anal anastomosis and a protective ileostomy. In 25 patients (6.4%), the procedure was performed under urgent conditions; in 137 patients (35%), the temporary ileostomy was omitted; in 117 patients (29.9%), the ileal pouch anal anastomosis was stapled. There was 1 hospital mortality (0.25%) and 1 30-day mortality. Mean length of stay was 9.2 +/- 5.6 days (3-68 days; median, 8 days) and was increased by the occurrence of septic complications (8.9 versus 13.6 days; P < 0.02) and by the omission of a temporary ileostomy (8.3 versus 10.4 days; P = 0.005). Complications included pelvic abscess (1.3%), anastomotic dehiscence (6.4%), bowel obstruction (11.7%), and anastomotic stenosis in need of mechanical dilatation (10.7%). Patients were asked to record their functional results on a questionnaire for 1 week at 3, 6, 9, 12, 18, and 24 months after the IPAA and yearly thereafter. Our data to 10 years show that median number of bowel movements (bms) was 6 bm/24 hours at all time intervals. The average number of bms increased by 0.3 bm/decade of life (P < 0.001). Throughout the entire follow-up, more than 75% of patients had at least 1 bm most nights, although fewer than 40% found it necessary to alter the time of their meals to avoid bms at inappropriate times. Depending on the time interval, between 57% and 78% of patients were always able to postpone a bm until convenient, and this ability was similar in patients with a stapled or hand-sewn ileoanal anastomosis; only up to 18% were able to always distinguish between flatus and stools, and this ability was similar in patients with a stapled or hand-sewn ileoanal anastomosis. Complete daytime and nighttime continence was achieved by 53-76% of patients depending on the time interval. The percentage of fully continent patients was higher following the stapled rather than the hand-sewn technique (P < 0.001), and this difference persisted over time. When patients experienced incontinence, its occurrence ameliorated over time (P < 0.001), and the occurrence of perianal rash and itching as well as the use of protective pads decreased over time (P < 0.008). At 5 years, patients judged quality of life as much better or better in 81.4% and overall satisfaction and overall adjustment as excellent or good in 96.3% and 97.5%, respectively.
Conclusions: We conclude that the IPAA confers a good quality of life. The majority of patients are fully continent, have 6 bms/d on average, and can defer a bm until convenient. When present, incontinence improves over time.
Figures
References
-
- Michelassi F, Stella M, Block GE. Prospective assessment of functional results after ileal J pouch—anal restorative proctocolectomy. Arch Surg. 1993;128:889-895. - PubMed
-
- Michelassi F, Block GE. A simplified technique for ileal J-pouch construction. Surg Gynecol Obstet. 1993;176:290-294. - PubMed
-
- Zeger SL, Liang KY. Longitudinal data analysis for discrete and continuous outcomes. Biometrics. 1986;42:121-130. - PubMed
-
- McIntyre PB, Pemberton JH, Wolff BG, et al. Comparing functional results one year and ten years after ileal pouch-anal anastomosis for chronic ulcerative colitis. Dis Colon Rectum. 1994;37:303-307. - PubMed
-
- Bullard KM, Madoff RD, Gemlo BT. Is ileoanal pouch function stable with time? Dis Colon Rectum. 2002;45:299-304. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
