

State of the art: why do the lungs of patients with cystic fibrosis become infected and why can't they clear the infection?
- PMID: 14511398
- PMCID: PMC203156
- DOI: 10.1186/1465-9921-4-8
State of the art: why do the lungs of patients with cystic fibrosis become infected and why can't they clear the infection?
Abstract
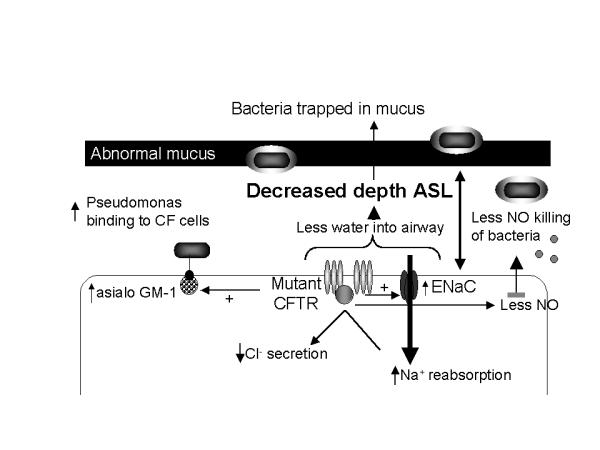
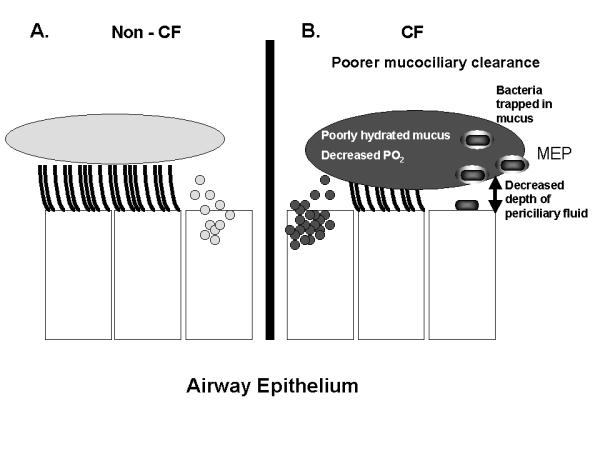
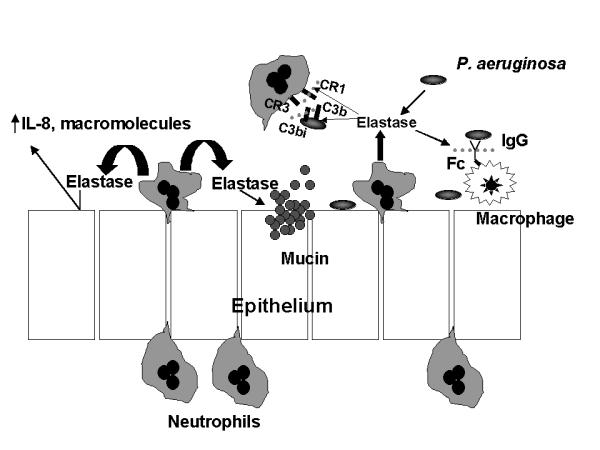
Cystic Fibrosis (CF) lung disease, which is characterized by airway obstruction, chronic bacterial infection, and an excessive inflammatory response, is responsible for most of the morbidity and mortality. Early in life, CF patients become infected with a limited spectrum of bacteria, especially P. aeruginosa. New data now indicate that decreased depth of periciliary fluid and abnormal hydration of mucus, which impede mucociliary clearance, contribute to initial infection. Diminished production of the antibacterial molecule nitric oxide, increased bacterial binding sites (e.g., asialo GM-1) on CF airway epithelial cells, and adaptations made by the bacteria to the airway microenvironment, including the production of virulence factors and the ability to organize into a biofilm, contribute to susceptibility to initial bacterial infection. Once the patient is infected, an overzealous inflammatory response in the CF lung likely contributes to the host's inability to eradicate infection. In response to increased IL-8 and leukotriene B4 production, neutrophils infiltrate the lung where they release mediators, such as elastase, that further inhibit host defenses, cripple opsonophagocytosis, impair mucociliary clearance, and damage airway wall architecture. The combination of these events favors the persistence of bacteria in the airway. Until a cure is discovered, further investigations into therapies that relieve obstruction, control infection, and attenuate inflammation offer the best hope of limiting damage to host tissues and prolonging survival.
Figures
References
-
- Davis PB, Drumm ML, Konstan MW. State of the Art: Cystic Fibrosis. Am J Resp Crit Care Med. 1996;154:1229–1256. - PubMed
-
- Lloyd-Still JD. Crohn's disease and cystic fibrosis. Dig Dis Sci. 1994;39:880–885. - PubMed
-
- Taylor CJ, Aswani N. The pancreas in cystic fibrosis. Paediatr Respir Rev. 2002;3:77–81. - PubMed
-
- Pilewski JM, Frizzell RA. Role of CFTR in airway disease. Physiol Rev. 1999;79(1 Suppl):S215–S255. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
