

Pathology and clinical relevance of radial scars: a review
- PMID: 14514771
- PMCID: PMC1770086
- DOI: 10.1136/jcp.56.10.721
Pathology and clinical relevance of radial scars: a review
Abstract
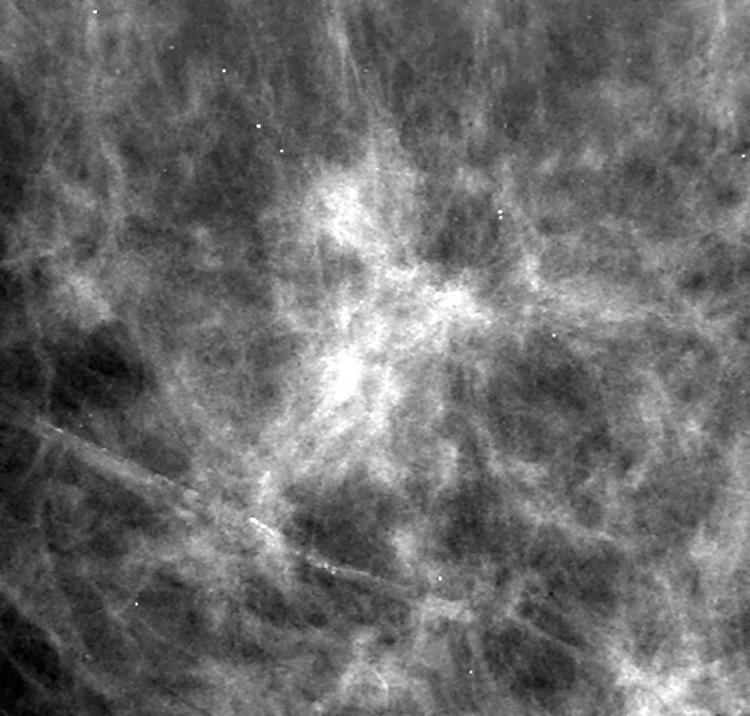
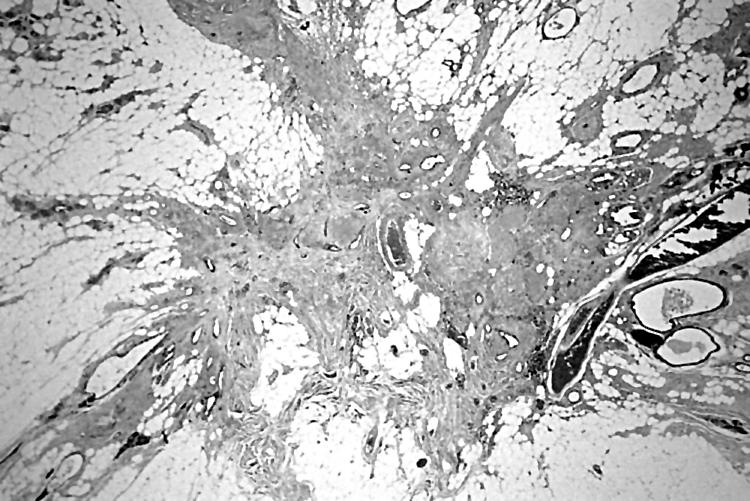
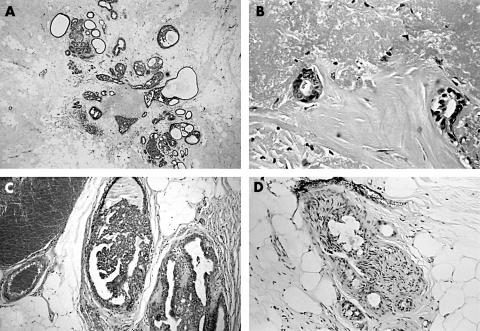
Radial scar (RS) is a benign, well recognised, radiological and pathological entity. Histologically, it is characterised by a fibroelastotic core with entrapped ducts and surrounding radiating ducts and lobules. Postmortem studies indicate that these lesions are present commonly in the population, especially in association with benign breast disease. In recent years, their clinical relevance has assumed more importance with the introduction of population based screening programmes. The exact pathogenesis of RS is unknown. Accumulating evidence indicates that they are associated with atypia and/or malignancy and, in addition, may be an independent risk factor for the development of carcinoma in either breast. In view of the association with atypia and malignancy, excision biopsy is justified in RS, although it has been argued that core biopsy evaluation and surveillance may be appropriate in selected patients.
Figures
References
-
- Fenoglio C, Lattes R. Sclerosing papillary proliferations in the female breast. A benign lesion often mistaken for carcinoma. Cancer 1974;33:691–700. - PubMed
-
- Azzopardi JG. Overdiagnosis of malignancy. In: Azzopardi JG, ed. Problems in breast pathology. Philadelphia: WB Saunders, 1979:167–91.
-
- Rickert RR, Kalisher L, Hutter RVP. Indurative mastopathy: a benign sclerosing lesion of breast with elastosis which may simulate carcinoma. Cancer 1981;47:561–71. - PubMed
-
- Tremblay G, Buell RH, Seemayer TA. Elastosis in benign sclerosing ductal proliferation of the female breast. Am J Surg Pathol 1977;1:155–9. - PubMed
-
- Fisher ER, Palekar AS, Kotwal N, et al. A nonencapsulated sclerosing lesion of the breast. Am J Clin Pathol 1979;71:240–6. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical