

Blood-spinal cord barrier after spinal cord injury: relation to revascularization and wound healing
- PMID: 14515352
- PMCID: PMC2837839
- DOI: 10.1002/jnr.10759
Blood-spinal cord barrier after spinal cord injury: relation to revascularization and wound healing
Abstract
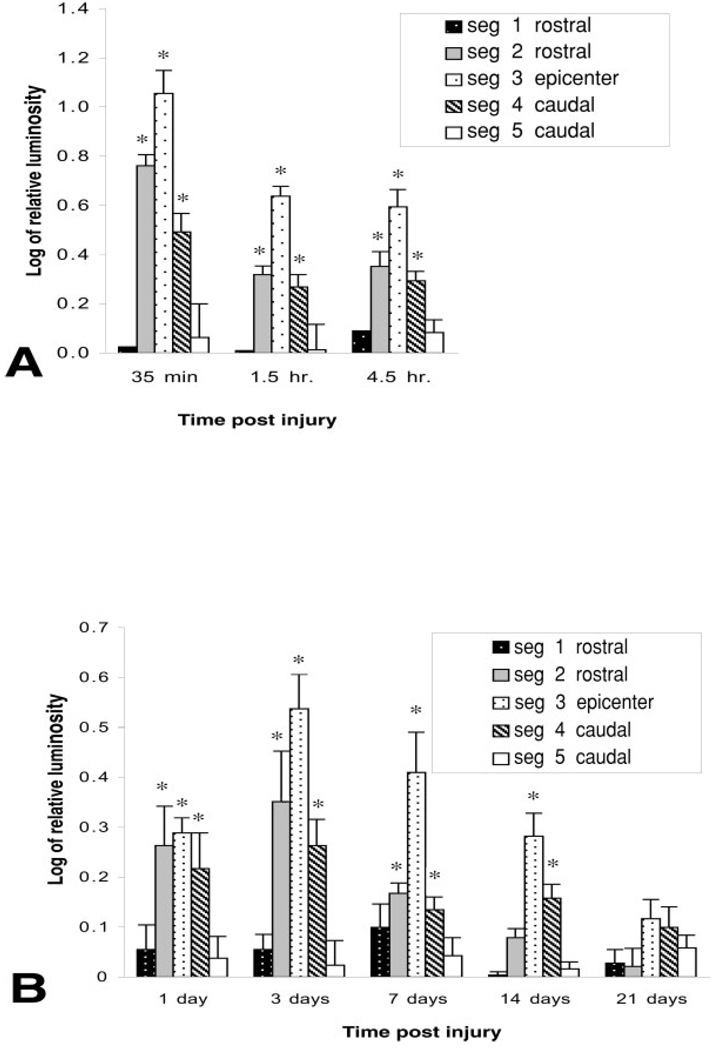
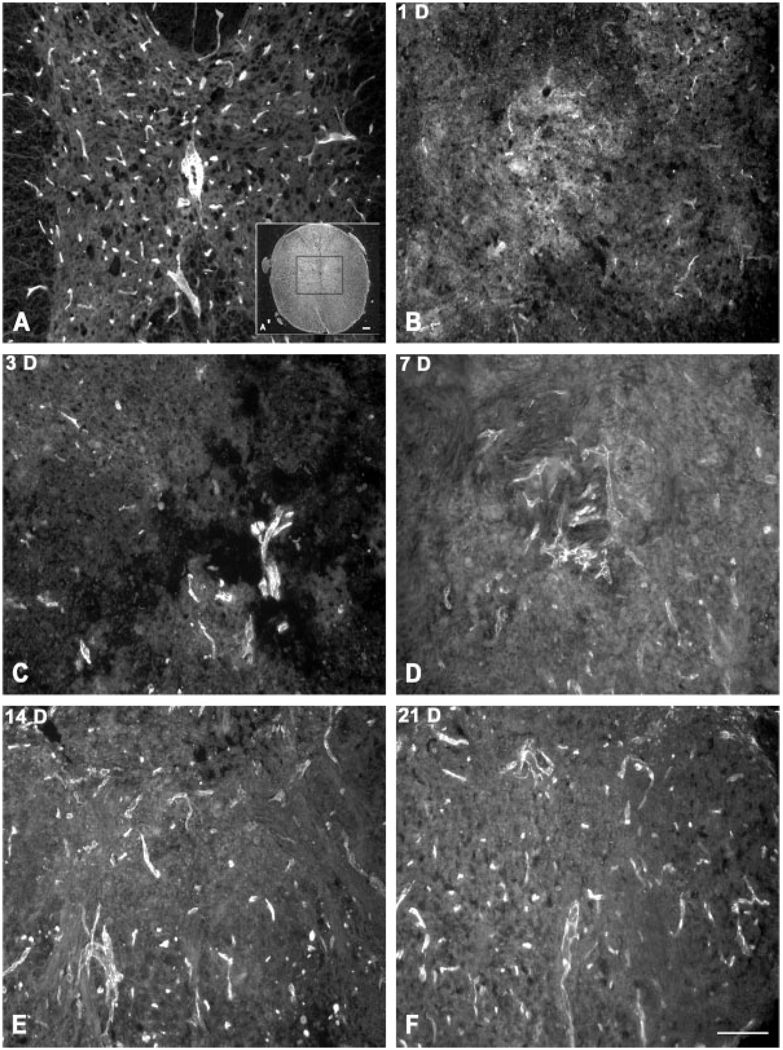
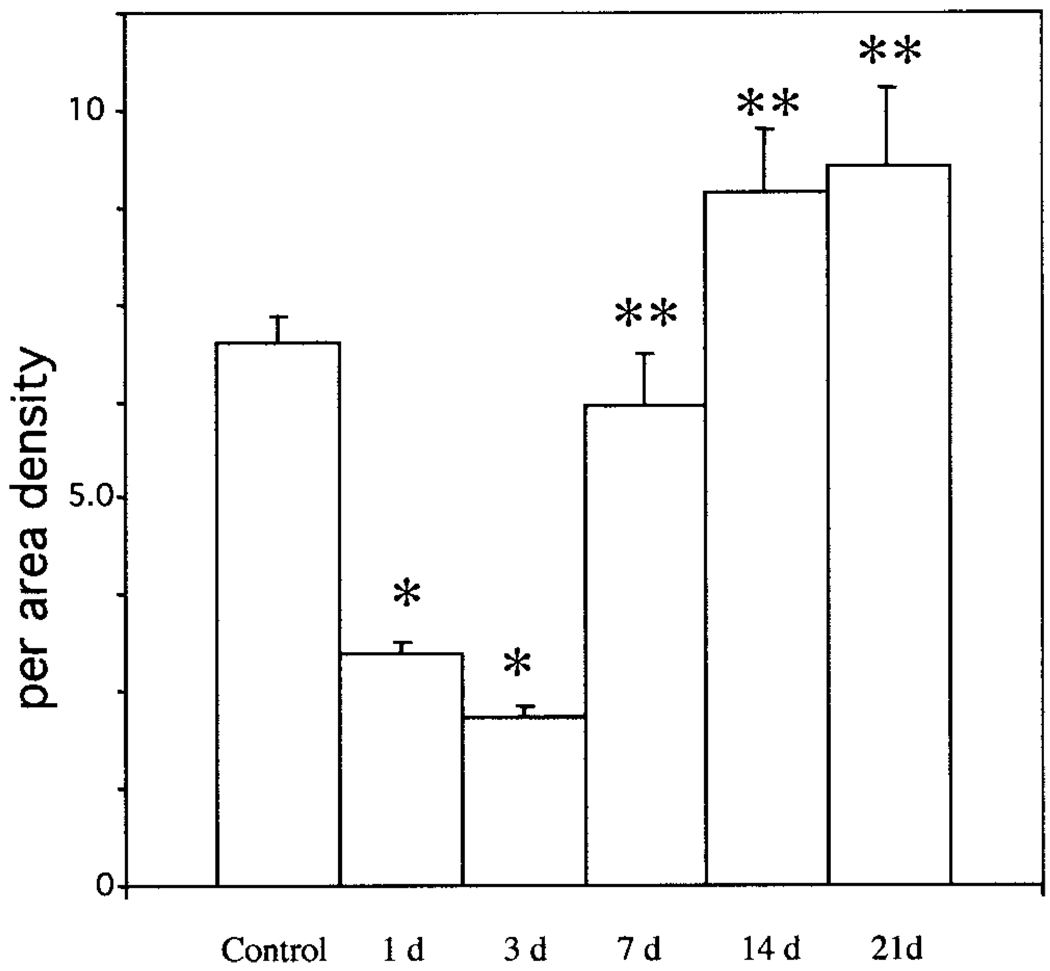
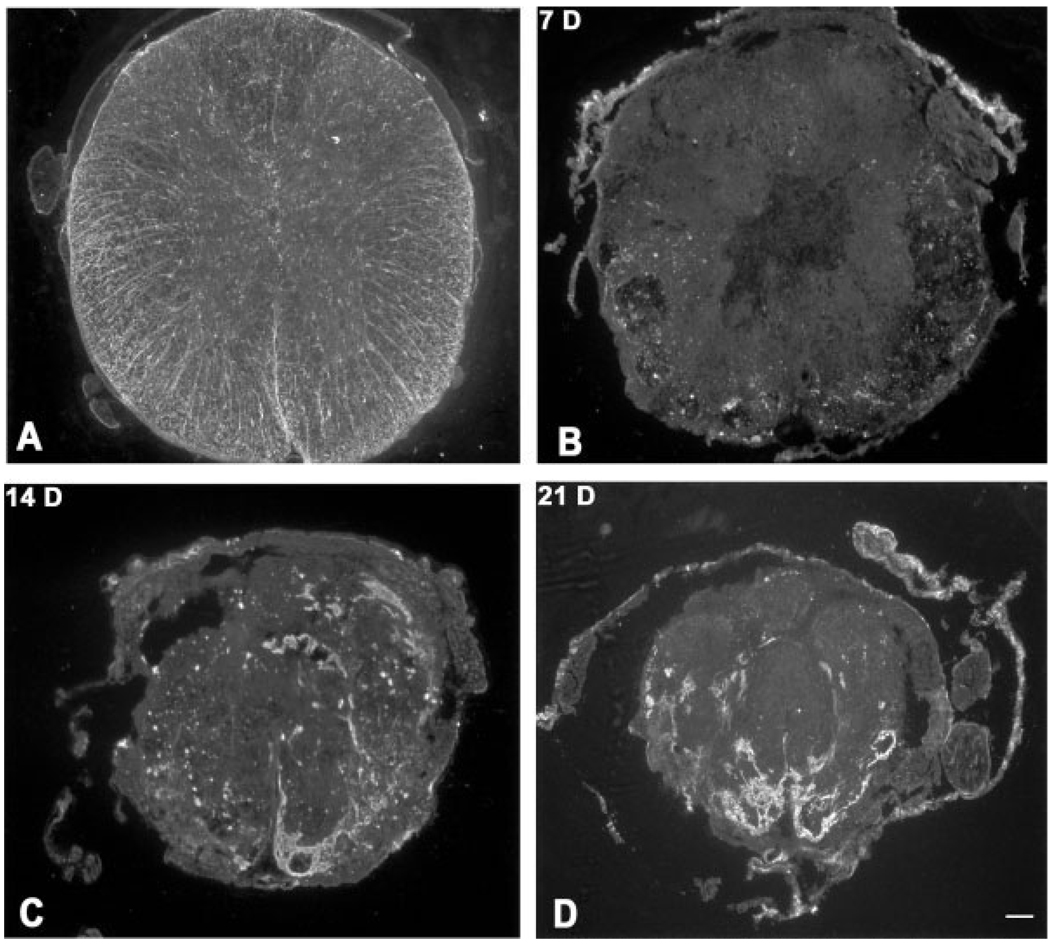
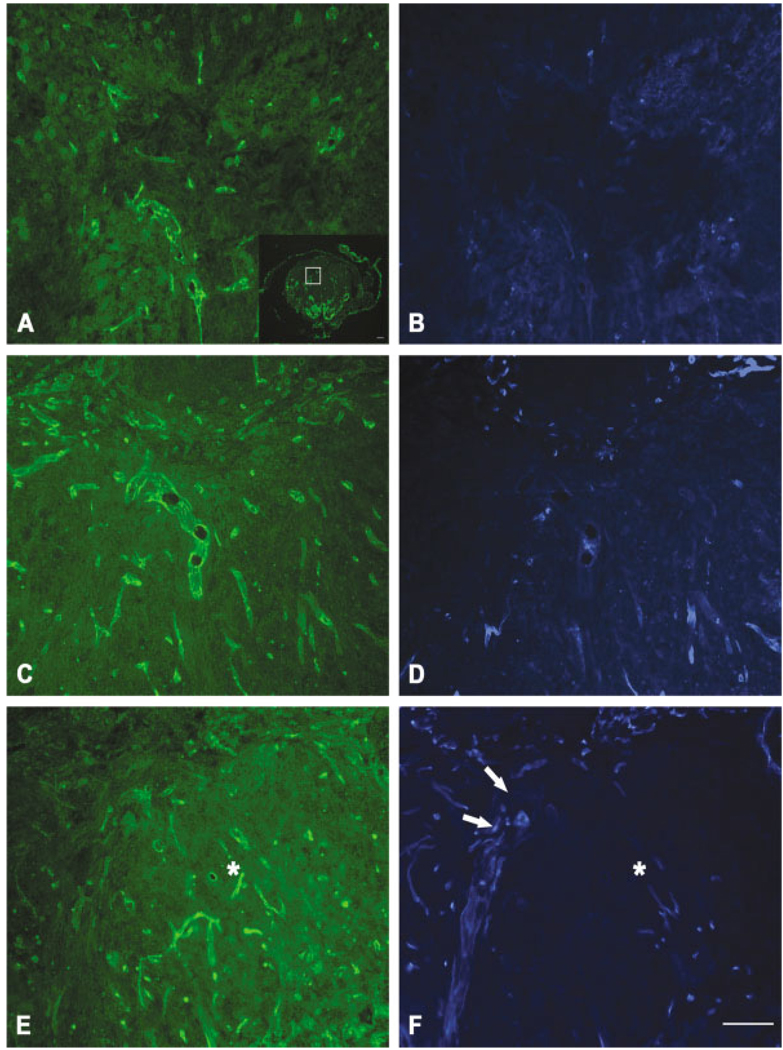
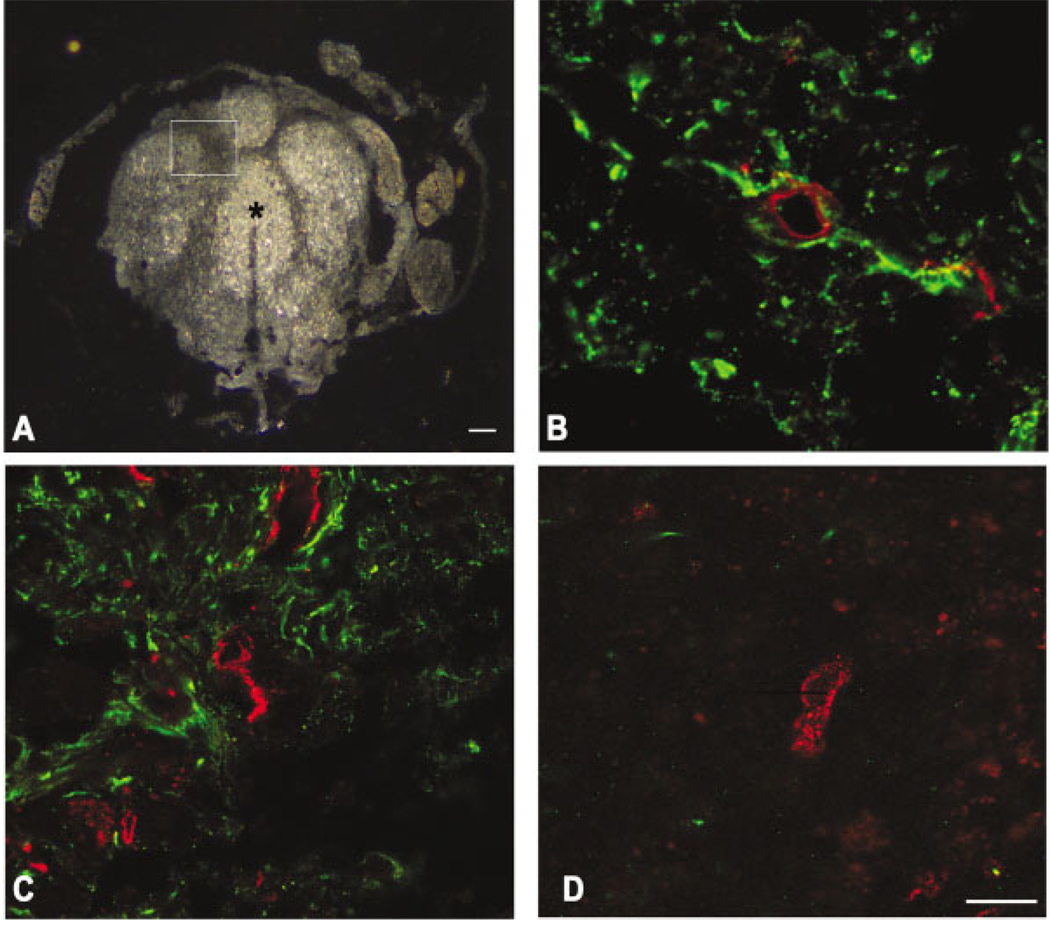
Spinal cord injury produces prominent disruption of the blood-spinal cord barrier. We have defined the blood-spinal cord barrier breakdown to the protein luciferase (61 kDa) in the acutely injured murine spinal cord and during revascularization. We show that newly formed and regenerating blood vessels that have abnormal permeability exhibit differential expression of the glucose-1 transporter (Glut-1), and that its expression is dependent on astrocytes. There was overt extravasation of luciferase within the first hour after injury, a period that coincided with marked tissue disruption within the epicenter of the lesion. Although there was a significant reduction in the number of blood vessels relative to controls by 24 hr after injury, abnormal barrier permeability remained significantly elevated. A second peak of abnormal barrier permeability at 3-7 days postinjury coincided with prominent revascularization of the epicenter. The barrier to luciferase was restored by 21 days postinjury and vascularity was similar to that of controls. During wound-healing process, the cord was reorganized into distinct domains. Between 14 and 21 days postinjury, each domain consisted primarily of nonneuronal cells, including macrophages. Astrocytes were limited characteristically to the perimeter of each domain. Only blood vessels affiliated closely with astrocytes in the perimeter expressed Glut-1, whereas blood vessels within each domain of the repairing cord did not express it. Together, these data demonstrate that both injured and regenerating vessels exhibit abnormal permeability and suggest that Glut-1 expression during revascularization is dependent on the presence of astrocytes.
Copyright 2003 Wiley-Liss, Inc.
Figures


References
-
- Beck DW, Roberts RL, Olson JJ. Glial cells influence membrane-associated enzyme activity at the blood-brain barrier. Brain Res. 1986;381:131–137. - PubMed
-
- Beck DW, Vinters HV, Hart MN, Cancilla PA. Glial cells influence polarity of the blood-brain barrier. J Neuropathol Exp Neurol. 1984;43:219–224. - PubMed
-
- Bilgen M, Abbe R, Narayana PA. Dynamic contrast-enhanced MRI of experimental spinal cord injury: in vivo serial studies. Magn Reson Med. 2001;45:614–622. - PubMed
-
- Bush TG, Puvanachandra N, Horner CH, Polito A, Ostenfeld T, Svendsen CN, Mucke L, Johnson MH, Sofroniew MV. Leukocyte infiltration, neuronal degeneration, and neurite outgrowth after ablation of scar-forming, reactive astrocytes in adult transgenic mice. Neuron. 1999;23:297–308. - PubMed
-
- Cancilla PA, Berliner J. Brain endothelial-astrocyte interactions. New York: Raven Press; 1993.
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
