

Diagnosis and management of benign paroxysmal positional vertigo (BPPV)
- PMID: 14517129
- PMCID: PMC202288
Diagnosis and management of benign paroxysmal positional vertigo (BPPV)
Abstract
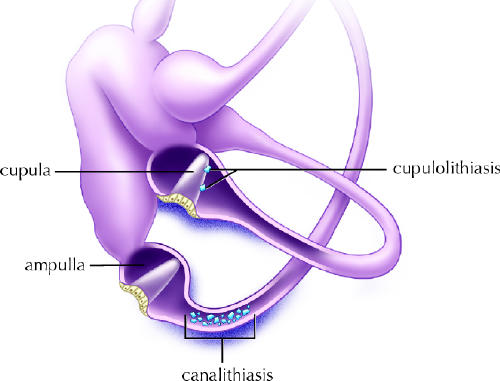
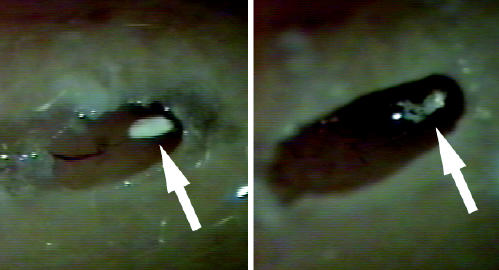
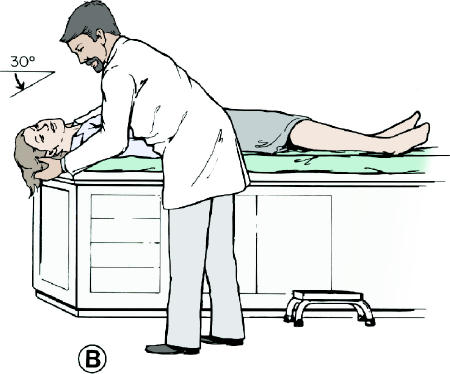
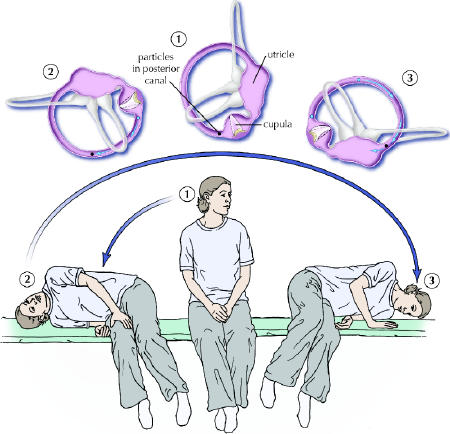
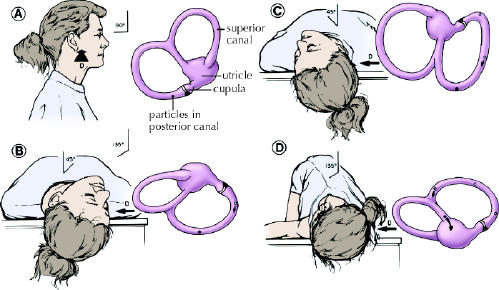
There is compelling evidence that free-floating endolymph particles in the posterior semicircular canal underlie most cases of benign paroxysmal positional vertigo (BPPV). Recent pathological findings suggest that these particles are otoconia, probably displaced from the otolithic membrane in the utricle. They typically settle in the dependent posterior canal and render it sensitive to gravity. Well over 90% of patients can be successfully treated with a simple outpatient manoeuvre that moves the particles back into the utricle. We describe the various techniques for this manoeuvre, plus treatments for uncommon variants of BPPV such as that of the lateral canal. For the rare patient whose BPPV is not responsive to these manoeuvres and has severe symptoms, posterior canal occlusion surgery is a safe and highly effective procedure.
Figures

References
-
- Katsarkas A. Benign paroxysmal positional vertigo (BPPV): idiopathic versus post-traumatic. Acta Otolaryngol 1999;119(7):745-9. - PubMed
-
- Bárány R. Diagnose von Krankheitserschernungen in Bereiche des Otolithenapparates. Acta Otolaryngol (Stockh) 1921;2:434-7.
-
- Dohlman G. Investigators in the function of the semicurcular canals. Acta Otolaryngol Suppl (Stockh) 1944;51:211.
-
- Hall SF, Ruby RR, McClure JA. The mechanics of benign paroxysmal vertigo. J Otolaryngol 1979;8(2):151. - PubMed
-
- Parnes LS, McClure JA. Free-floating endolymph particles: a new operative finding during posterior semicircular canal occlusion. Laryngoscope 1992; 102 (9):988-92. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical