

Seroprevalence of human papillomavirus-16, -18, -31, and -45 in a population-based cohort of 10000 women in Costa Rica
- PMID: 14520455
- PMCID: PMC2394308
- DOI: 10.1038/sj.bjc.6601272
Seroprevalence of human papillomavirus-16, -18, -31, and -45 in a population-based cohort of 10000 women in Costa Rica
Abstract
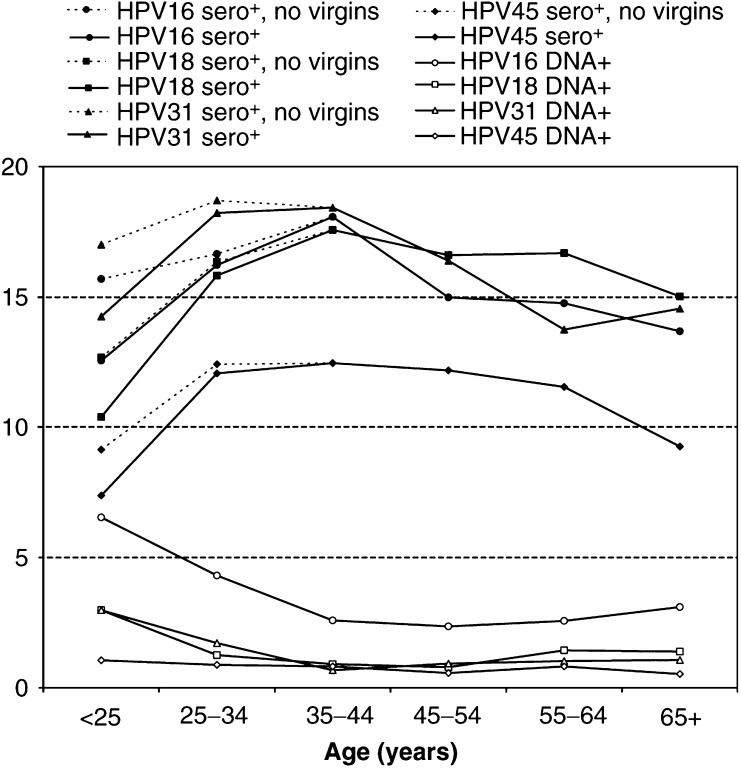
Human papillomavirus (HPV) seroprevalence and determinants of seropositivity were assessed in a 10049-woman population-based cohort in Guanacaste, Costa Rica. Serologic responses based on VLP-based ELISA were obtained from the plasma collected at study enrollment in 1993/1994 for HPV-16 (n=9949), HPV-18 (n=9928), HPV-31 (n=9932), and HPV-45 (n=3019). Seropositivity was defined as five standard deviations above the mean optical density obtained for studied virgins (n=573). HPV-16, -18, -31, and -45 seroprevalence was 15, 15, 16, and 11%, respectively. Of women DNA-positive for HPV-16, -18, -31, or -45, seropositivity was 45, 34, 51, and 28%, respectively. Peak HPV seroprevalence occurred a decade after DNA prevalence; lifetime number of sexual partners was the key determinant of seropositivity independent of DNA status and age. DNA- and sero-positive women showed the highest risk for concurrent CIN3/cancer, followed by DNA-positive, sero-negative women.
Figures
References
-
- Andersson-Ellstrom A, Dillner J, Hagmar B, Schiller J, Sapp M, Forssman L, Milsom I (1996) Comparison of development of serum antibodies to HPV-16 and HPV33 and acquisition of cervical HPV DNA among sexually experienced and virginal young girls A longitudinal cohort study. Sex Transm Dis 23: 234–238 - PubMed
-
- Bosch FX, Manos MM, Munoz N, Sherman M, Jansen AM, Peto J, Schiffman MH, Moreno V, Kurman R, Shah KV (1995) Prevalence of human papillomavirus in cervical cancer: a worldwide perspective. International biological study on cervical cancer (IBSCC) Study Group. J Natl Cancer Inst 87: 796–802 - PubMed
-
- Carter JJ, Koutsky LA, Hughes JP, Lee SK, Kuypers J, Kiviat N, Galloway DA (2000) Comparison of human papillomavirus types 16, 18, and 6 capsid antibody responses following incident infection. J Infect Dis 181: 1911–1919 - PubMed
-
- Carter JJ, Koutsky LA, Wipf GC, Christensen ND, Lee SK, Kuypers J, Kiviat N, Galloway DA (1996) The natural history of human papillomavirus type 16 capsid antibodies among a cohort of university women. J Infect Dis 174: 927–936 - PubMed
-
- Castle PE, Schiffman M, Gravitt PE, Kendall H, Fishman S, Dong H, Hildesheim A, Herrero R, Bratti MC, Sherman ME, Lorincz A, Schussler JE, Burk RD (2002a) Comparisons of HPV DNA detection by MY09/11 PCR methods. J Med Virol 68: 417–423 - PubMed
