

Diagnosis of axillary nodal metastases by ultrasound-guided core biopsy in primary operable breast cancer
- PMID: 14520465
- PMCID: PMC2394321
- DOI: 10.1038/sj.bjc.6601290
Diagnosis of axillary nodal metastases by ultrasound-guided core biopsy in primary operable breast cancer
Abstract
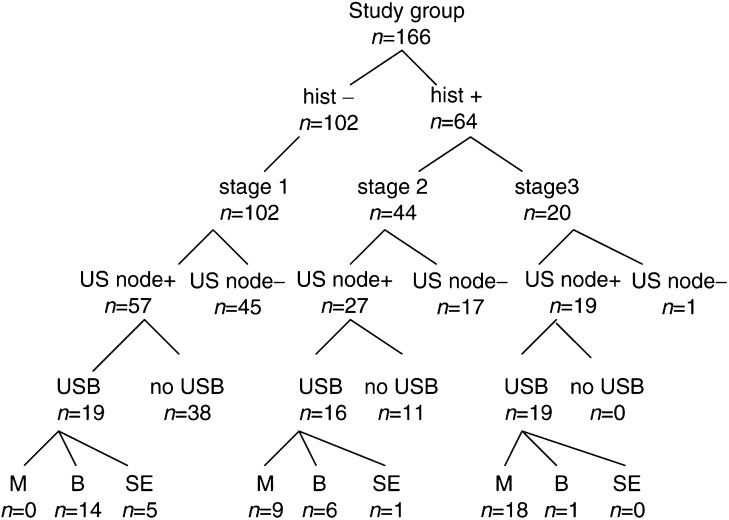
The purpose of this study was to examine the use of ultrasound (US)-guided core biopsy of axillary nodes in patients with operable breast cancer. The ipsilateral axillae of 187 patients with suspected primary operable breast cancer were scanned. Nodes were classified based on their shape and cortical morphology. Abnormal nodes underwent US-guided core biopsy/fine needle aspiration (FNA), and the results correlated with subsequent axillary surgery. The nodes were identified on US in 103 of 166 axillae of patients with confirmed invasive carcinoma. In total, 54 (52%) met the criteria for biopsy: 48 core biopsies (26 malignant, 20 benign node, two normal) and six FNA were performed. On subsequent definitive histological examination, 64 of 166 (39%) had axillary metastases. Of the 64 patients with involved nodes at surgery, preoperative US identified nodes in 46 patients (72%), of which 35 (55%) met the criteria for biopsy and 27 (42%) of these were diagnosed preoperatively by US-guided biopsy. In conclusion, US can identify abnormal nodes in patients presenting with primary operable breast cancer. In all, 65% of these nodes are malignant and this can often be confirmed with US-guided core biopsy.
Figures
References
-
- Bonnema J, van Geel AN, van Ooijen B, Mali SPM, Tjiam LS, Henzen-Logmans SC, Schmitz PIM, Wiggers T (1997) Ultrasound guided aspiration biopsy for detection of non palpable axillary node metastases in breast cancer patients: New diagnostic method. World J Surg 21: 270–274 - PubMed
-
- Britton PD, McCann J (1999) Needle biopsy in the NHS Breast Screening Programme 1996/1997: how much and how accurate? Breast 8: 5–11
-
- Bruneton JN, Caramella E, Hery M, Aubanel D, Manzino JJ, Picard JL (1986) Axillary lymph node metastases in breast cancer: preoperative detection with US. Radiology 158: 325–326 - PubMed
-
- De Kanter AY, van Eijck CHJ, van Geel AN, Kruijt RH, Henzen SC, Paul MA, Eggermont AMM, Wiggers T (1999) Multicentre study of ultrasonographically guided axillary node biopsy in patients with breast cancer. Br J Surg 86: 1459–1462 - PubMed
-
- Duff M, Hill AD, Mc Greal G, Walsh S, Mc Dermott EW, O'Higgins NJ (2001) Prospective evaluation of the morbidity of axillary clearance. Br J Surg 88(6): 891 - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
