

Review of evidence and explanations for suboptimal screening and treatment of dyslipidemia in women. A conceptual model
- PMID: 14521649
- PMCID: PMC1494935
- DOI: 10.1046/j.1525-1497.2003.20910.x
Review of evidence and explanations for suboptimal screening and treatment of dyslipidemia in women. A conceptual model
Abstract
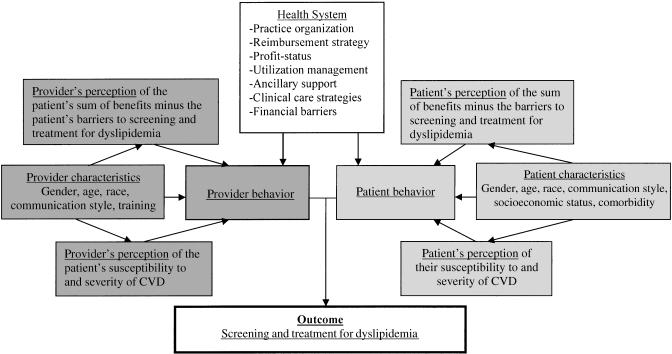
Screening and treatment rates for dyslipidemia in populations at high risk for cardiovascular disease (CVD) are inappropriately low and rates among women may be lower than among men. We conducted a review of the literature for possible explanations of these observed gender differences and categorized the evidence in terms of a conceptual model that we describe. Factors related to physicians' attitudes and knowledge, the patient's priorities and characteristics, and the health care systems in which they interact are all likely to play important roles in determining screening rates, but are not well understood. Research and interventions that simultaneously consider the influence of patient, clinician, and health system factors, and particularly research that focuses on modifiable mechanisms, will help us understand the causes of the observed gender differences and lead to improvements in cholesterol screening and management in high-risk women. For example, patient and physician preferences for lipid and other CVD risk factor management have not been well studied, particularly in relation to other gender-specific screening issues, costs of therapy, and by degree of CVD risk; better understanding of how available health plan benefits interact with these preferences could lead to structural changes in benefits that might improve screening and treatment.
Figures
Similar articles
-
Waist circumference predicts cardiometabolic and global Framingham risk among women screened during National Woman's Heart Day.J Womens Health (Larchmt). 2006 Jan-Feb;15(1):24-34. doi: 10.1089/jwh.2006.15.24. J Womens Health (Larchmt). 2006. PMID: 16417415
-
Sex disparity in the management of dyslipidemia among patients with type 2 diabetes mellitus in a managed care organization.Am J Manag Care. 2005 Feb;11(2):69-73. Am J Manag Care. 2005. PMID: 15726854
-
Gender disparities in the quality of cardiovascular disease care in private managed care plans.Womens Health Issues. 2007 May-Jun;17(3):120-30. doi: 10.1016/j.whi.2007.03.002. Epub 2007 Apr 19. Womens Health Issues. 2007. PMID: 17448685
-
Gender-related differences in the impact of tropical diseases on women: what do we know?J Biosoc Sci. 1994 Jan;26(1):37-53. doi: 10.1017/s0021932000021040. J Biosoc Sci. 1994. PMID: 8200878 Review.
-
[Mammography and cervical cancer screening--a systematic review about women's knowledge, attitudes and participation in Germany].Gesundheitswesen. 2012 Nov;74(11):722-35. doi: 10.1055/s-0031-1286271. Epub 2011 Oct 19. Gesundheitswesen. 2012. PMID: 22012563 German.
Cited by
-
An Update on Gender Disparities in Coronary Heart Disease Care.Curr Atheroscler Rep. 2016 May;18(5):28. doi: 10.1007/s11883-016-0574-5. Curr Atheroscler Rep. 2016. PMID: 27029220 Review.
-
Quality of cardiovascular disease preventive care and physician/practice characteristics.J Gen Intern Med. 2006 Mar;21(3):231-7. doi: 10.1111/j.1525-1497.2006.00331.x. J Gen Intern Med. 2006. PMID: 16637822 Free PMC article.
-
Response by sex to statin plus ezetimibe or statin monotherapy: a pooled analysis of 22,231 hyperlipidemic patients.Lipids Health Dis. 2011 Aug 22;10:146. doi: 10.1186/1476-511X-10-146. Lipids Health Dis. 2011. PMID: 21859459 Free PMC article.
-
Impact of performance improvement continuing medical education on cardiometabolic risk factor control: the COSEHC initiative.J Contin Educ Health Prof. 2014 Winter;34(1):25-36. doi: 10.1002/chp.21217. J Contin Educ Health Prof. 2014. PMID: 24648361 Free PMC article.
-
Association between facility characteristics and the process of care delivered to patients with hepatitis C virus infection.Dig Dis Sci. 2014 Feb;59(2):273-81. doi: 10.1007/s10620-013-2773-z. Epub 2013 Aug 10. Dig Dis Sci. 2014. PMID: 23934366
References
-
- American Heart Association. American Heart Association 2002 Heart and Stroke Statistical Update. Dallas, TX: American Heart Association; 2001. pp. 1–38.
-
- Miettinen T, Pyorala K, Olsson A, et al. Cholesterol-lowering therapy in women and elderly patients with myocardial infarction or angina pectoris. Circulation. 1997;96:4211–8. - PubMed
-
- McPherson R, Genest J, Angus C, Murray P. The Women's Atorvastatin Trial on Cholesterol (WATCH): frequency of achieving NCEP-II target LDL-C levels in women with and without established CVD. Am Heart J. 2001;141:949–56. - PubMed
-
- LIPID Study Group. Prevention of cardiovascular events and death with pravastatin in patients with coronary heart disease and a broad range of initial cholesterol levels. N Engl J Med. 1998;339:1349–57. - PubMed
-
- Lewis S, Sacks F, Mitchell J, et al. Effect of pravastatin on cardiovascular events in women after myocardial infarction. The Cholesterol and Recurrent Events (CARE) trial. J Am Coll Cardiol. 1998;32:140–6. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical