

Minimally invasive esophagectomy: outcomes in 222 patients
- PMID: 14530720
- PMCID: PMC1360107
- DOI: 10.1097/01.sla.0000089858.40725.68
Minimally invasive esophagectomy: outcomes in 222 patients
Abstract
Objective: To assess our outcomes after minimally invasive esophagectomy (MIE).
Summary background data: Esophagectomy has traditionally been performed by open methods. Results from most series include mortality rates in excess of 5% and hospital stays frequently greater than 10 days. MIE has the potential to improve these results, but only a few small series have been reported. This report summarizes our experience of 222 cases.
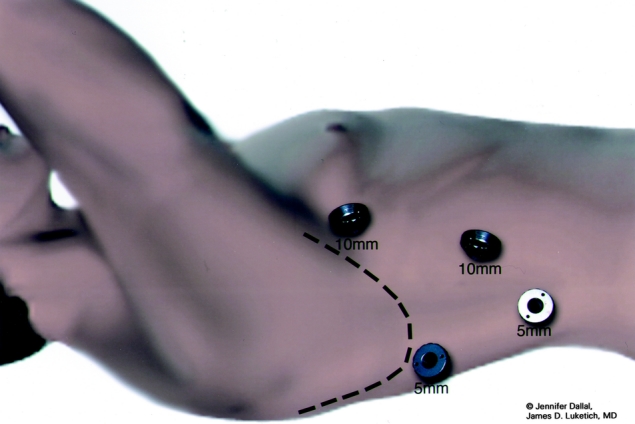
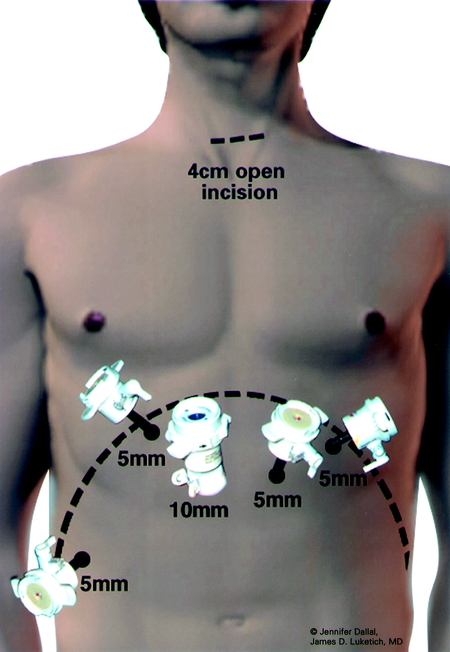
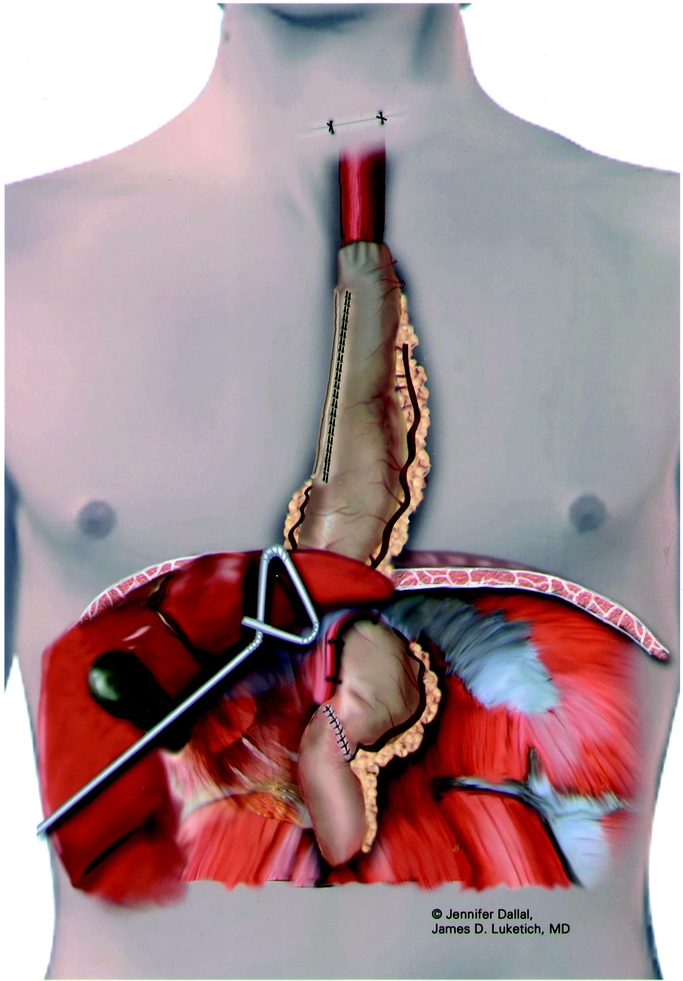
Methods: From 1996 to 2002, MIE was performed in 222 patients. Indications for operation included high-grade dysplasia (n = 47) and cancer (n = 175). Neoadjuvant chemotherapy was used in 78 (35.1%) and radiation in 36 (16.2%). Initially, a laparoscopic transhiatal approach was used (n = 8), but subsequently our approach evolved to include thoracoscopic mobilization (n = 214).
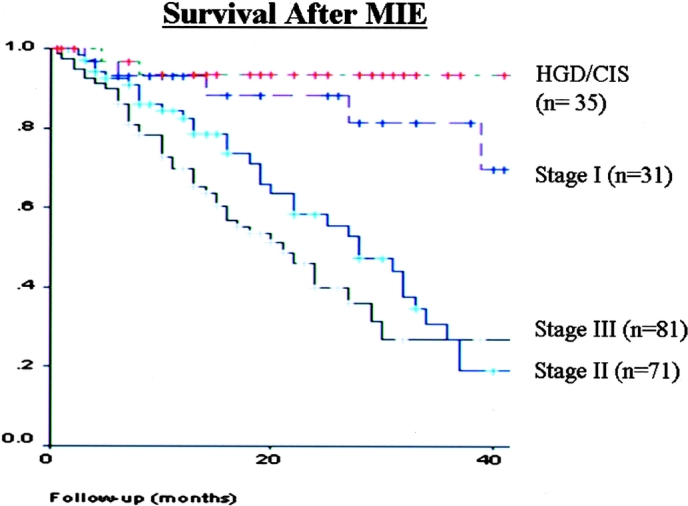
Results: There were 186 men and 36 women. Median age was 66.5 years (range, 39-89). Nonemergent conversion to open procedure was required in 16 patients (7.2%). MIE was successfully completed in 206 (92.8%) patients. The median intensive care unit stay was 1 day (range, 1-30); hospital stay was 7 days (range, 3-75). Operative mortality was 1.4% (n = 3). Anastomotic leak rate was 11.7% (n = 26). At a mean follow-up of 19 months (range, 1-68), quality of life scores were similar to preoperative values and population norms. Stage specific survival was similar to open series.
Conclusions: MIE offers results as good as or better than open operation in our center with extensive minimally invasive and open experience. In this single institution experience, we observed a lower mortality rate (1.4%) and shorter hospital stay (7 days) than most open series. Given these results, we are now developing an intergroup trial (ECOG 2202) to assess MIE in a multicenter setting.
Figures

References
-
- Kelsen DP, Ginsberg R, Pajak TF, et al. Chemotherapy followed by surgery compared with surgery alone for localized esophageal cancer. N Engl J Med. 1998;339:1979-1984. - PubMed
-
- Birkmeyer JD, Siewers AE, Finlayson EVA, et al. Hospital volume and surgical mortality in the United States. N Engl J Med. 2002;346:1128-1137. - PubMed
-
- Overholt BF, Panjehpour M, Ayres M. Photodynamic therapy for Barrett's esophagus: cardiac effects. Lasers Surg Med. 1997;21:317-320. - PubMed
-
- Fernando HC, Luketich JD, Beunaventura PO, et al. Outcomes of minimally invasive esophagectomy (MIE) for high-grade dysplasia of the esophagus EJCTS. 2002;22:1-6. - PubMed
-
- Dallemagne B, Weerts JM, Jehaes C, et al. Laparoscopic Nissen fundoplication: preliminary report. Surg Laparosc Percut Tech. 1991;1:138-143. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
