

Laparoscopic retroperitoneal lymph node dissection in the extremely obese patient: technical insight into access and port placement
- PMID: 14558718
- PMCID: PMC3113209
Laparoscopic retroperitoneal lymph node dissection in the extremely obese patient: technical insight into access and port placement
Abstract
Purpose: We report on laparoscopic retroperitoneal lymph node dissection (RPLND) in a morbidly obese patient to discuss the associated technical steps for satisfactory completion of staging lymphadenectomy.
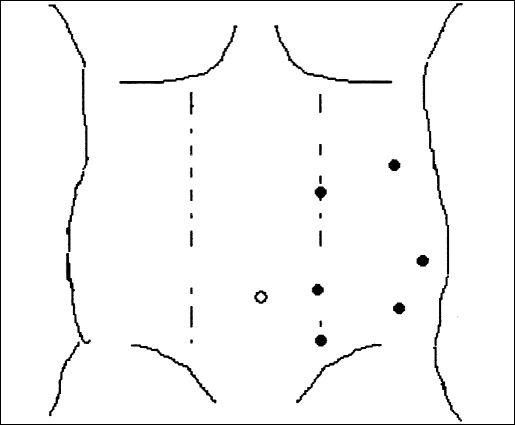
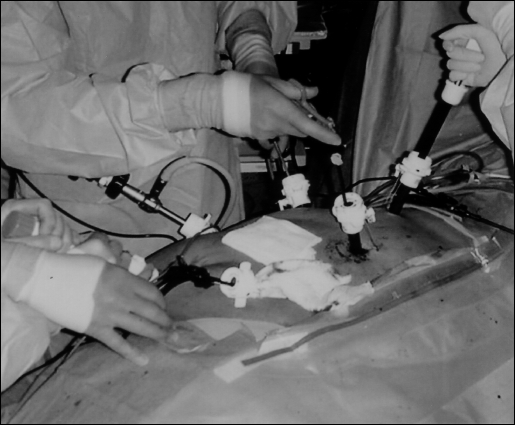
Methods: A laparoscopic RPLND was performed using a modified template on the left side. Initially, 4 ports were placed with the patient in the supine position. Three were placed 3 cm to the left of midline and one in the anterior axillary line, at the level of the umbilicus. During the operation, successful bowel retraction necessitated placement of 2 additional ports in the anterior axillary line (just above the pelvis and off the tip of the 12th rib). Using these 6 trocar sites, the dissection was completed, and 44 lymph nodes were obtained.
Results: Laparoscopic retroperitoneal lymph node dissection was accomplished in an extremely obese patient with acceptable morbidity by using prudent modification of standard techniques.
Conclusion: If access and port placement limitations are overcome, the benefits of laparoscopy in the obese are clear. This report serves as a signpost that laparoscopic retroperitoneal lymph node dissection for testes cancer can also be accomplished using modification of standard techniques.
Figures
Similar articles
-
Laparoscopic retroperitoneal lymph node dissection for nonseminomatous germ cell tumors: indications and limitations.J Urol. 1996 Sep;156(3):1108-13. J Urol. 1996. PMID: 8709319 Clinical Trial.
-
Laparoscopic RPLND for clinical stage I nonseminomatous germ cell testicular cancer: current status.Urol Oncol. 2004 Mar-Apr;22(2):145-8. doi: 10.1016/j.urolonc.2004.01.006. Urol Oncol. 2004. PMID: 15082014 Review.
-
Laparoscopic retroperitoneal lymph node dissection for clinical stage I nonseminomatous germ cell testicular cancer: a long-term update.Urology. 2003 Aug;62(2):324-7. doi: 10.1016/s0090-4295(03)00324-8. Urology. 2003. PMID: 12893344
-
Robot-assisted Laparoscopic Retroperitoneal Lymph Node Dissection for Testicular Cancer: Evolution of the Technique.Eur Urol. 2016 Oct;70(4):661-667. doi: 10.1016/j.eururo.2016.03.031. Epub 2016 Apr 5. Eur Urol. 2016. PMID: 27068395
-
Indications, evolving technique, and early outcomes with robotic retroperitoneal lymph node dissection.Curr Opin Urol. 2018 Sep;28(5):461-468. doi: 10.1097/MOU.0000000000000530. Curr Opin Urol. 2018. PMID: 29979235 Review.
Cited by
-
Trans- and extraperitoneal retroperitoneal lymph node dissection (RPLND) in the treatment for nonseminomatous germ cell testicular tumors (NSGCT): a single Chinese center's retrospective analysis.Int Urol Nephrol. 2014 Feb;46(2):363-9. doi: 10.1007/s11255-013-0547-3. Epub 2013 Sep 1. Int Urol Nephrol. 2014. PMID: 23996573
References
-
- Janetschek G, Hobisch A, Peschel R, Hittmair A, Bartsch G. Laparoscopic retroperitoneal lymph node dissection for stage I nonseminomatous testicular carcinoma: long-term outcome. J Urol. 2000;163(6):1793–1796 - PubMed
-
- Childers JM, Hatch KD, Tran AN, Surwit EA. Laparoscopic para-aortic lymphadenectomy in gynecologic malignancies. Obstet Gynecol. 1993;82(5):741–747 - PubMed
-
- Holub Z, Bartos P, Jabor A, Eim J, Fischlova D, Kliment L. Laparoscopic surgery in obese women with endometrial cancer. J Am Assoc Gynecol Laparosc. 2000;7(1):83–88 - PubMed
-
- Curet MJ. Special problems in laparoscopic surgery: previous abdominal surgery, obesity, and pregnancy. Surg Clin N Am. 2000;80(4):1093–1109 - PubMed
-
- Robinson SP, Hirtle M, Imbrie JZ, Moore MM. The mechanics underlying laparoscopic intra-abdominal surgery for obese patients. J Laparoendosc Adv Surg Tech. 1998;8(1):11–18 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical