

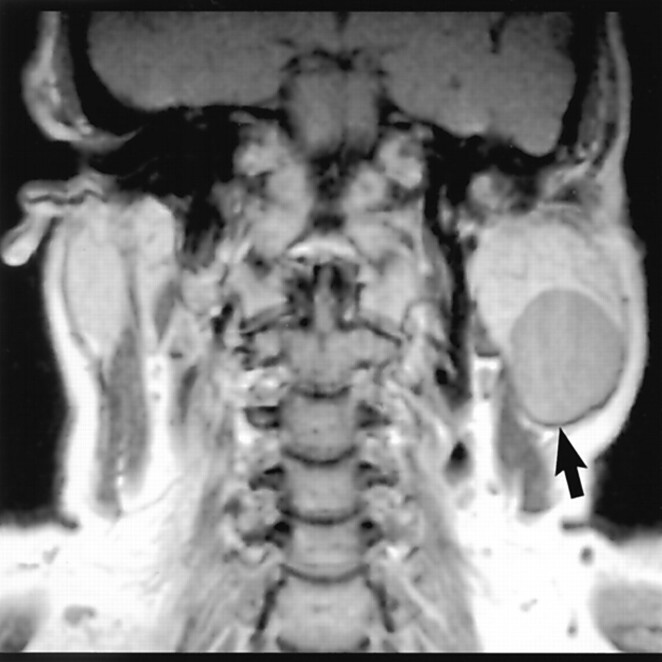
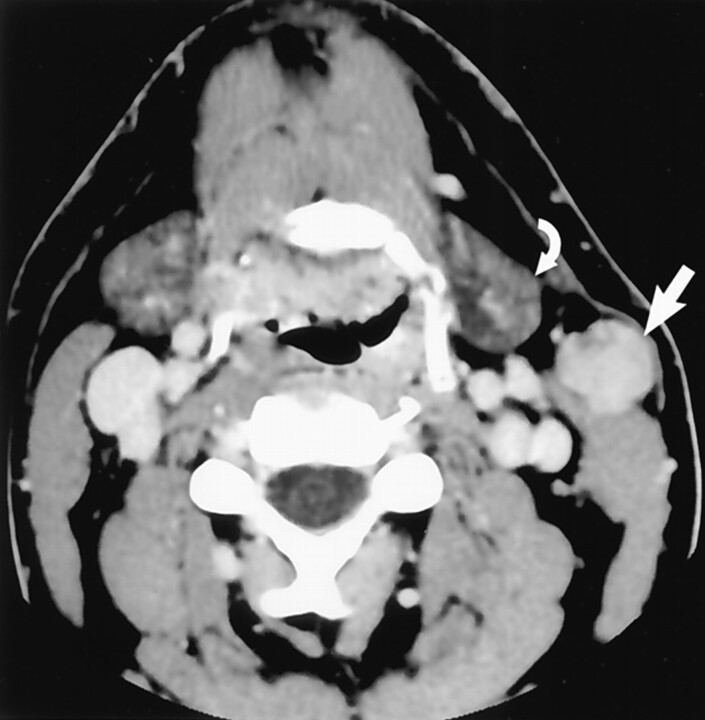
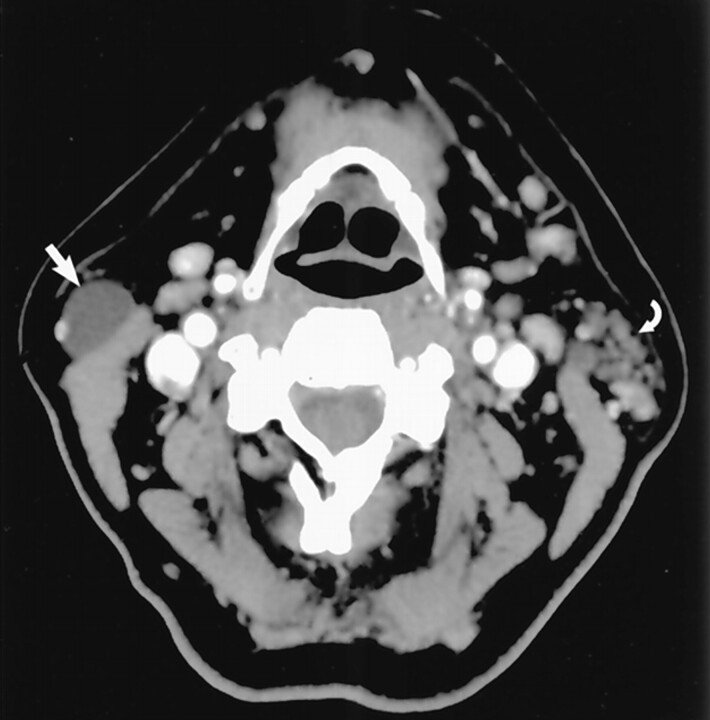
Earring lesions of the parotid tail
Abstract
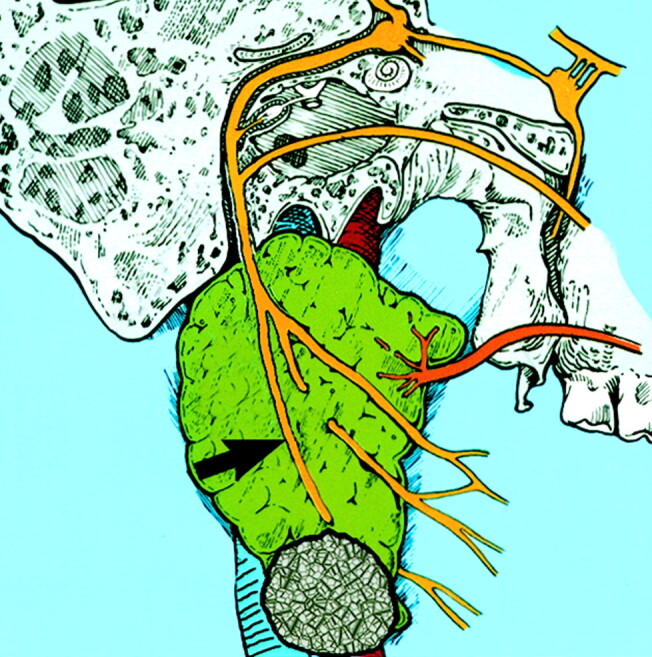
Background and purpose: Masses in the parotid tail can be a source of consternation to radiologists and clinicians; inaccurate localization may lead to significant iatrogenic complication. We sought to review the pertinent anatomic localizing features of the parotid tail, relevant facial nerve anatomy, and sources of clinical and radiologic confusion. To conclude, we review imaging features that are helpful in generating a diagnosis in this location.
Methods: We retrospectively reviewed the imaging and clinical features of 111 parotid tail masses in 103 patients (56 male, 45 female, two of unknown sex; age range, 5 months-81 years). The following imaging findings were noted: size, enhancement, multiplicity of lesions, attenuation on CT scans, signal intensity on MR images, and appearance of the surrounding parotid gland. Diagnosis was confirmed by either surgical resection or biopsy findings or by specific clinical data or characteristic imaging findings.
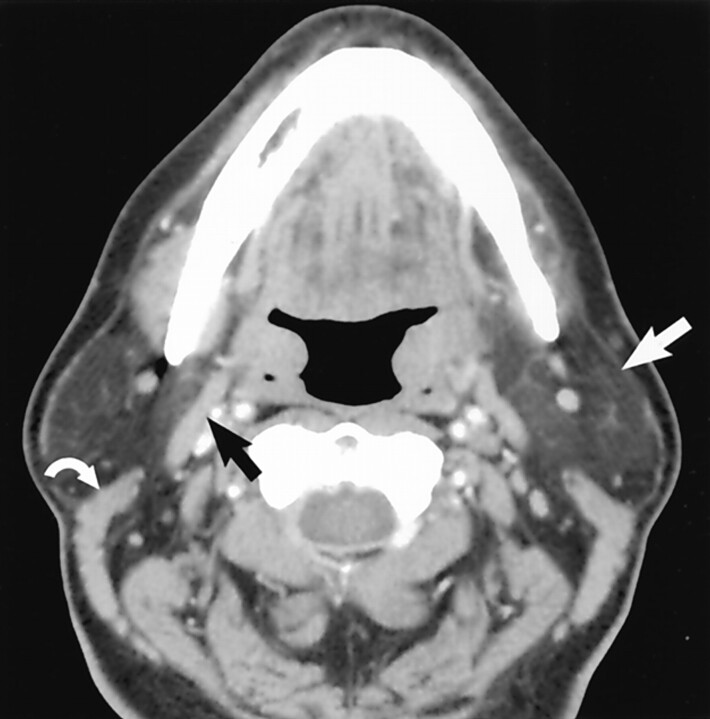
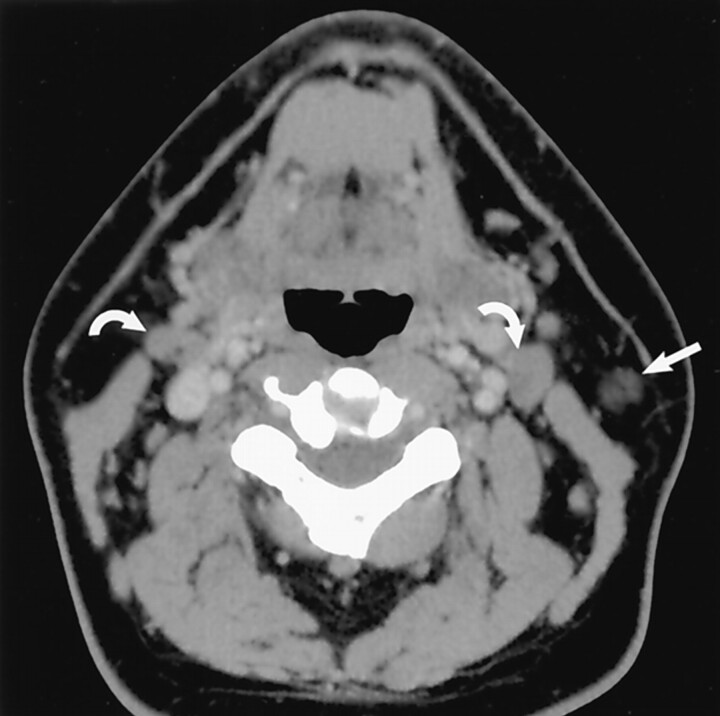
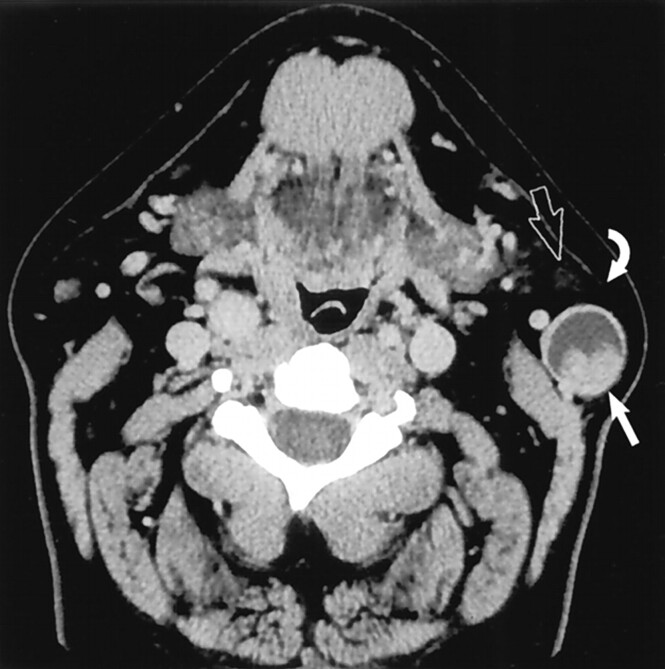
Results: Seventeen types of parotid tail masses were identified. Benign lesions were: pleomorphic adenoma (n = 15), Warthin tumor (n = 14), infectious process (n = 13), venous malformation (n = 9), and Sjögren disease (n = 9), lymphatic malformations (n = 7), lipoma (n = 6), HIV lymphoepithelial lesion (n = 4), first brachial cleft cyst (n = 3), oncocytoma (n = 2), sarcoid (n = 1), and lymph node (n = 1). Malignant lesions were: Non-Hodgkin lymphoma (n = 14), metastatic disease (n = 7), mucoepidermoid carcinoma (n = 4), acinic cell carcinoma (n = 1), and undifferentiated carcinoma (n = 1). Eight patients had two diagnoses.
Conclusion: Understanding normal parotid tail anatomy is important to radiologists, because accurate localization has implications for appropriate management of masses in this location, potentially reducing the occurrence of marginal mandibular nerve injury.
Figures


References
-
- Harnsberger HR. Head and Neck Digital Teaching File. Salt Lake City, UT: Amirsys, Inc.;2002
-
- Bannister LH. Alimentary system. In: Williams PL, Bannister L, Berry M, et al, eds. Gray’s Anatomy: The Anatomical Basis of Medicine and Surgery. 38th ed. Edinburgh, Scotland: Churchill Livingstone1995. :1691–1692
-
- Som PM, Brandwein M. Salivary glands. In: Som PM, Curtin HD, eds. Head and Neck Imaging. 3rd ed, vol 2. St. Louis, MO: Mosby-Year Book, Inc.;1996. :824–830, 898–907
-
- Hoffman H, Funk G, Endres D. Evaluation and surgical treatment of tumors of the salivary glands. In: Thawley SE, Panje W, Batsakis L, Robert J, eds. Comprehensive Management of Head and Neck Tumors. 2nd ed, vol 2. Philadelphia, PA: W. B. Saunders Company;1999. :1147–1177
-
- Gates G, Johns M. Embryology and anatomy of the salivary glands. In: Paparella MM, Shumrick D, eds. Otolaryngology: Basic Sciences and Related Disciplines. 2nd ed, vol 1. Philadelphia, PA: W. B. Saunders Company;1980. :150–151
MeSH terms
LinkOut - more resources
Full Text Sources