

Postchemoembolisation syndrome--tumour necrosis or hepatocyte injury?
- PMID: 14562011
- PMCID: PMC2394347
- DOI: 10.1038/sj.bjc.6601329
Postchemoembolisation syndrome--tumour necrosis or hepatocyte injury?
Abstract
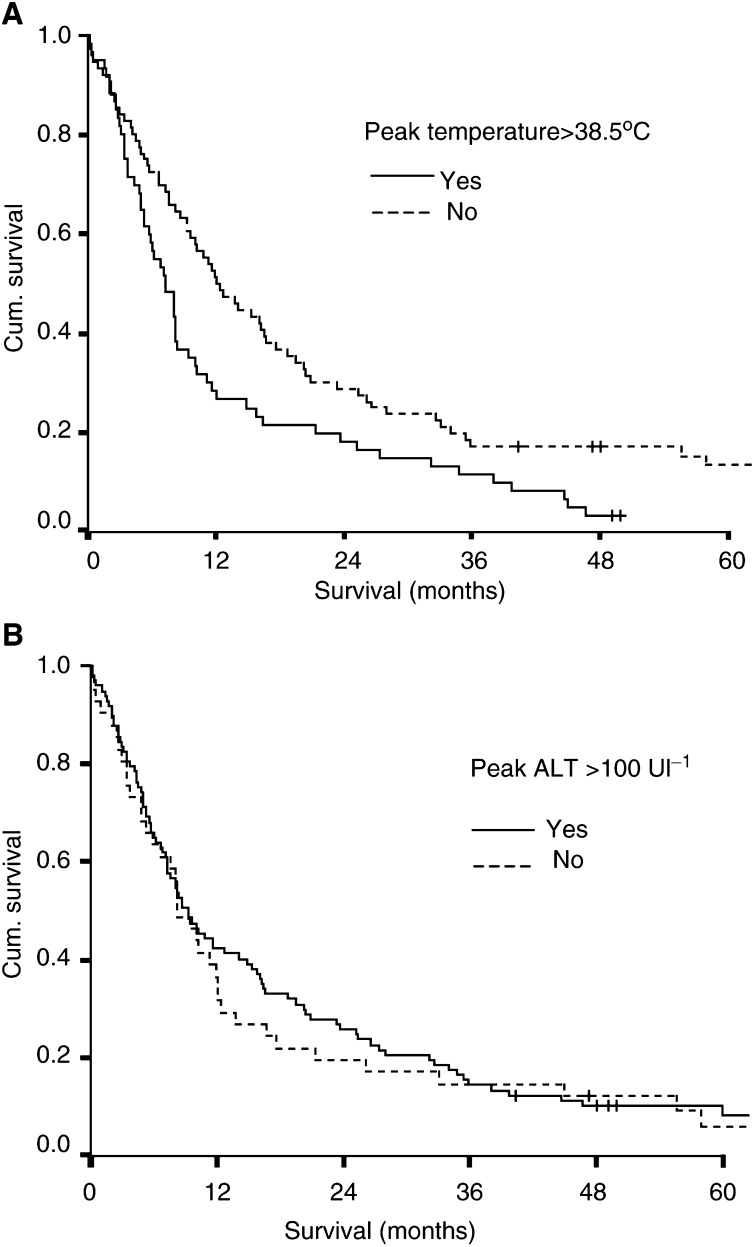
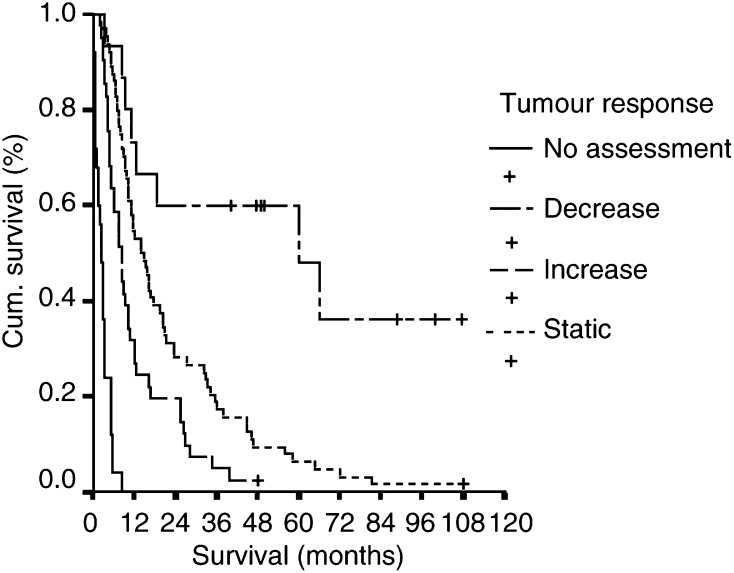
Transarterial chemoembolisation of liver tumours is typically followed by elevated body temperature and liver transaminase enzymes. This has often been considered to indicate successful embolisation. The present study questions whether this syndrome reflects damage to tumour cells or to the normal hepatic tissue. The responses to 256 embolisations undertaken in 145 patients subdivided into those with hepatocyte-derived (primary hepatocellular carcinoma) and nonhepatocyte-derived tumours (secondary metastases) were analysed to assess the relative effects of tumour necrosis and damage to normal hepatocytes in each group. Cytolysis, measured by elevated alanine aminotransferase, was detected in 85% of patients, and there was no difference in the abnormalities in liver function tests measured between the two groups. Furthermore, cytolysis was associated with a higher rate of postprocedure symptoms and side effects, and elevated temperature was associated with a worse survival on univariate analysis. Multivariate analysis demonstrated that there was no benefit in terms of survival from having elevated temperature or cytolysis following embolisation. Cytolysis after chemoembolisation is probably due to damage to normal hepatocytes. Temperature changes may reflect tumour necrosis or necrosis of the healthy tissue. There is no evidence that either a postchemoembolisation fever or cytolysis is associated with an enhanced tumour response or improved long-term survival in patients with primary or secondary liver cancer.
Figures
References
-
- Bismuth H, Morino M, Sherlock D, Castaing D, Miglietta C, Cauquil P, Roche A (1992) Primary treatment of hepatocelllar carcinoma by arterial chemoembolization. Am J Surg 163: 387–394 - PubMed
-
- Castells A, Bruix J, Ayuso C, Brù C, Montanyà X, Boix L, Rodes J (1995) Transarterial embolization for hepatocellular carcinoma. Antibiotic prophylaxis and clinical meaning of postembolization fever. J Hepatol 22: 410–415 - PubMed
-
- Chung JW, Park JH, Han JK, Choi BI, Han MC, Lee HS, Kim CY (1996) Hepatic tumours: predisposing factors for complications of transcatheter oily chemoembolization. Radiology 198: 33–40 - PubMed
-
- Groupe d'Etude de la traitment du Carcinome Hepatocellulaire (1995) A comparison of lipiodol chemoembolization and conservative treatment for unresectable hepatocellular carcinoma. New Engl J Med 332: 1256–1261 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
