

Montelukast and fluticasone compared with salmeterol and fluticasone in protecting against asthma exacerbation in adults: one year, double blind, randomised, comparative trial
- PMID: 14563743
- PMCID: PMC218809
- DOI: 10.1136/bmj.327.7420.891
Montelukast and fluticasone compared with salmeterol and fluticasone in protecting against asthma exacerbation in adults: one year, double blind, randomised, comparative trial
Abstract
Objectives: To assess the effect of montelukast versus salmeterol added to inhaled fluticasone propionate on asthma exacerbation in patients whose symptoms are inadequately controlled with fluticasone alone. Design and setting A 52 week, two period, double blind, multicentre trial during which patients whose symptoms remained uncontrolled by inhaled corticosteroids were randomised to add montelukast or salmeterol.
Participants: Patients (15-72 years; n = 1490) had a clinical history of chronic asthma for > or = 1 year, a baseline forced expiratory volume in one second (FEV1) value 50-90% predicted, and a beta agonist improvement of > or = 12% in FEV1.
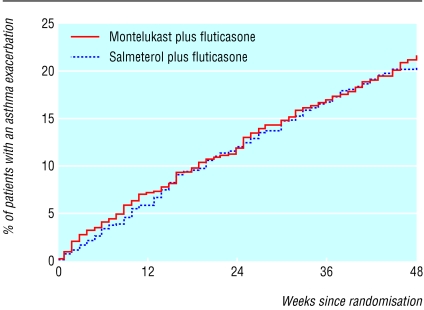
Main outcome measures: The primary end point was the percentage of patients with at least one asthma exacerbation.
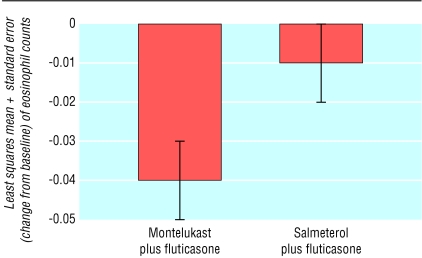
Results: 20.1% of the patients in the group receiving montelukast and fluticasone had an asthma exacerbation compared with 19.1% in the group receiving salmeterol and fluticasone; the difference was 1% (95% confidence interval -3.1% to 5.0%). With a risk ratio (montelukast-fluticasone/salmeterol-fluticasone) of 1.05 (0.86 to 1.29), treatment with montelukast and fluticasone was shown to be non-inferior to treatment with salmeterol and fluticasone. Salmeterol and fluticasone significantly increased FEV1 before a beta agonist was used and morning peak expiratory flow compared with montelukast and fluticasone (P < or = 0.001), whereas FEV1 after a beta agonist was used and improvements in asthma specific quality of life and nocturnal awakenings were similar between the groups. Montelukast and fluticasone significantly (P = 0.011) reduced peripheral blood eosinophil counts compared with salmeterol and fluticasone. Both treatments were generally well tolerated.
Conclusion: The addition of montelukast in patients whose symptoms remain uncontrolled by inhaled fluticasone could provide equivalent clinical control to salmeterol.
Figures
References
-
- National Institutes of Health, National Heart, Lung and Blood Institute. Asthma management and prevention. Global initiative for asthma. A practical guide for public health officials and health care professionals. Based on the global strategy for asthma management and prevention NHLBI/WHO workshop report. Bethesda, MD: NIH, 1995. (NIH publication No. 96-3659A.) Updated report 2002. www.ginasthma.com (accessed 28 Aug 2003).
-
- British asthma guidelines coordinating committee. British guidelines on asthma management: 1995 review and position statement. Thorax 1997;52: S1-24.
-
- Barnes PJ. Efficacy of inhaled corticosteroids in asthma. J Allergy Clin Immunol 1998;102: 531-8. - PubMed
-
- Greening A, Wind P, Northfield M, Shaw G. Added salmeterol versus higher-dose corticosteroid in asthma patients with symptoms on existing inhaled corticosteroids. Lancet 1994;344: 219-24. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical