

Network organization of interstitial connective tissue cells in the human endolymphatic duct
- PMID: 14566021
- PMCID: PMC3957558
- DOI: 10.1177/002215540305101109
Network organization of interstitial connective tissue cells in the human endolymphatic duct
Abstract
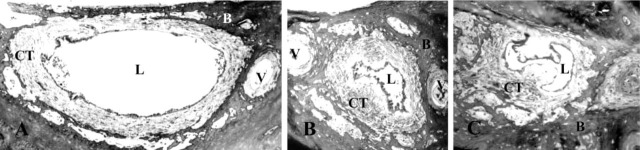
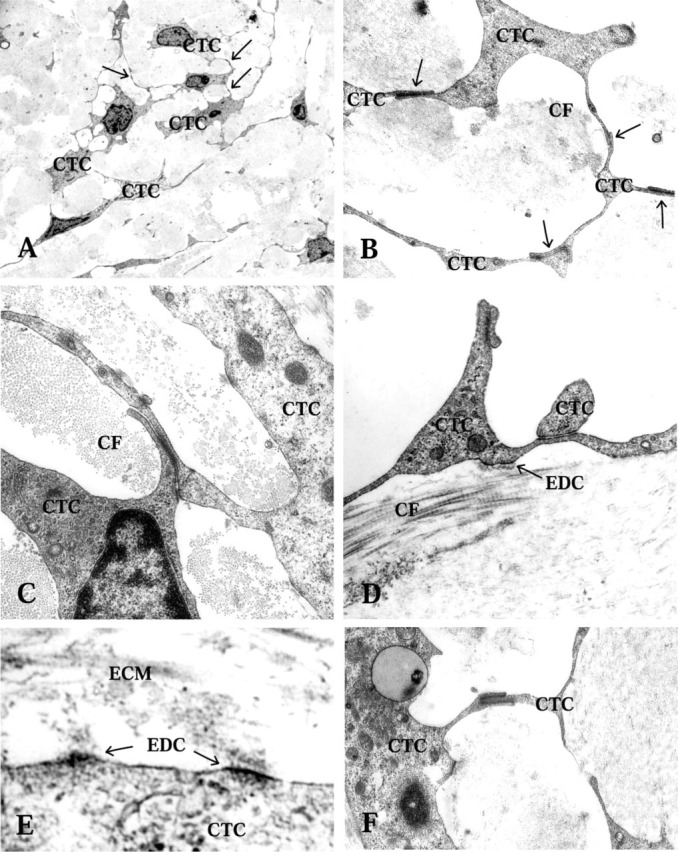
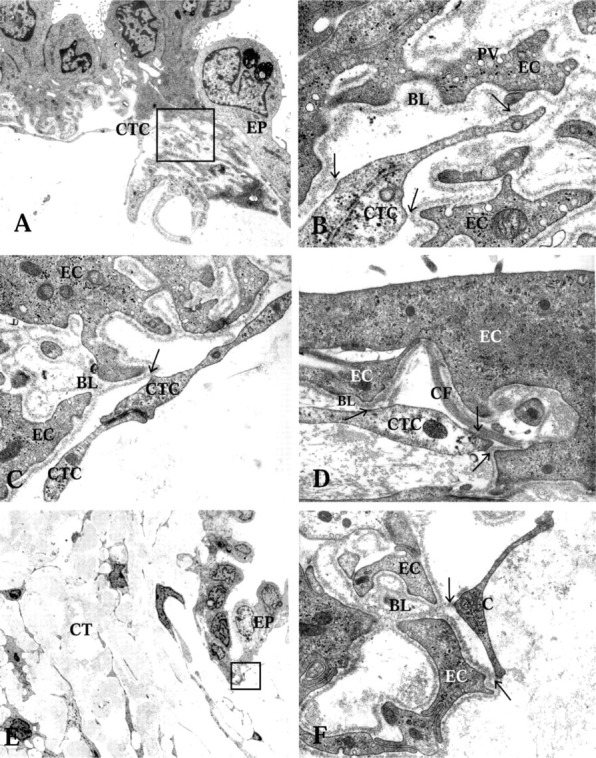
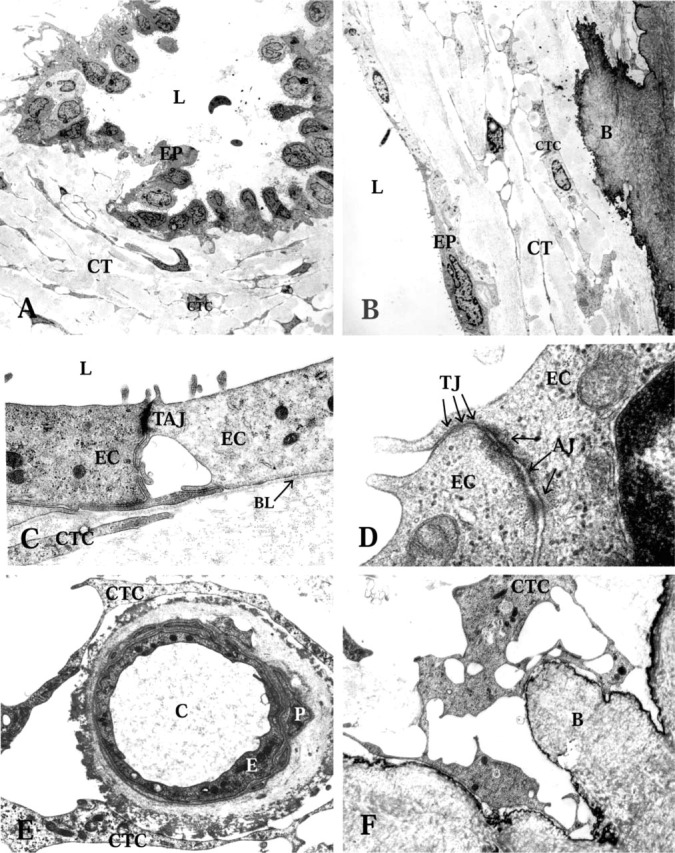
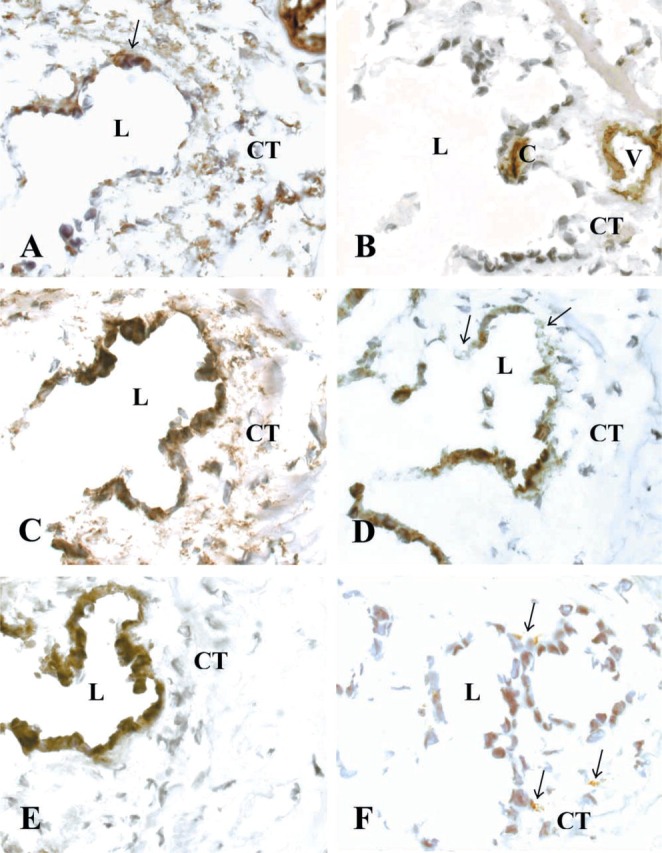
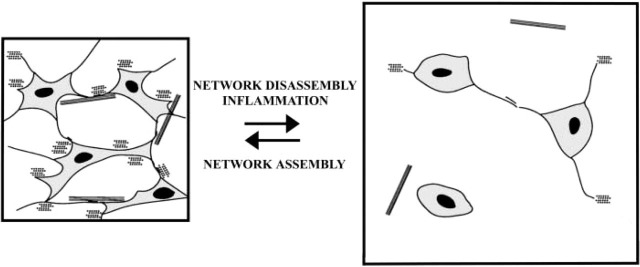
The human endolymphatic duct (ED) and sac of the inner ear have been suggested to control endolymph volume and pressure. However, the physiological mechanisms for these processes remain obscure. We investigated the organization of the periductal interstitial connective tissue cells and extracellular matrix (ECM) in four freshly fixed human EDs by transmission electron microscopy and by immunohistochemistry. The unique surgical material allowed a greatly improved structural and epitopic preservation of tissue. Periductal connective tissue cells formed frequent intercellular contacts and focally occurring electron-dense contacts to ECM structures, creating a complex tissue network. The connective tissue cells also formed contacts with the basal lamina of the ED epithelium and the bone matrix, connecting the ED with the surrounding bone of the vestibular aqueduct. The interstitial connective tissue cells were non-endothelial and non-smooth muscle fibroblastoid cells. We suggest that the ED tissue network forms a functional mechanical entity that takes part in the control of inner ear fluid pressure and endolymph resorption.
Figures
References
-
- Altermatt HJ, Gebbers JO, Muller C, Arnold W, Laissue JA. (1990) Human endolymphatic sac: evidence for a role in inner ear immune defence. ORL J Otorhinolaryngol Relat Spec 52:143–148 - PubMed
-
- Bagger-Sjöbäck D, Rask-Andersen H. (1986) The permeability barrier of the endolymphatic sac. A hypothesis of fluid and electrolyte exchange based on freeze fracturing. Am J Otol 7:134–140 - PubMed
-
- Bauwens LJ, De Groot JC, Ramaekers FC, Linthicum F, Veldman JE, Huizing EH. (1991) Differential immunohistochemical detection of cytokeratins and vimentin in the surgically removed human endolymphatic duct and sac. Eur Arch Otorhinolaryngol 248:495–501 - PubMed
-
- Berg A, Ekwall A-KH, Rubin K, Stjernschantz J, Reed RK. (1998) Effect of PGE1, PGI2, and PGF2 alpha analogs on collagen gel compaction in vitro and interstitial pressure in vivo. Am J Physiol 274:H663–671 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
