

Occult pneumothorax in the mechanically ventilated trauma patient
- PMID: 14577712
- PMCID: PMC3211710
Occult pneumothorax in the mechanically ventilated trauma patient
Abstract
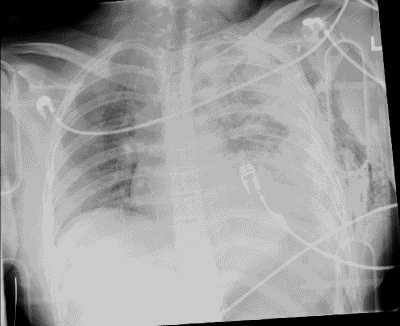
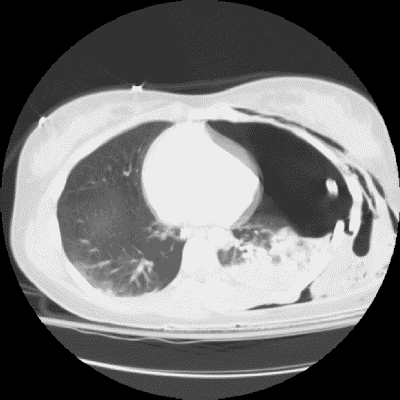
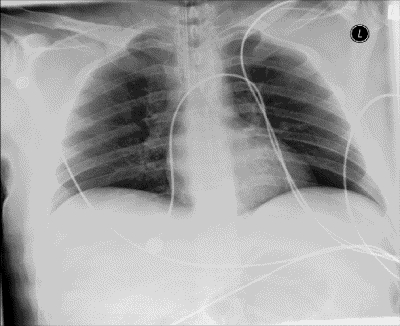
The term occult pneumothorax (OP) describes a pneumothorax that is not suspected on the basis of clinical examination or plain radiography but is ultimately detected with thoracoabdominal computed tomography (CT). This situation is increasingly common in trauma care with the increased use of CT. The rate is approximately 5% in injured people presenting to hospital, with CT revealing at least twice as many pneumothoraces as suspected on plain radiography. Whereas pneumothorax is a common and treatable cause of mortality and morbidity, there is substantial disagreement regarding the appropriate treatment of OP. The greatest controversy is in patients in the critical care unit who require positive-pressure ventilation. There is little current evidence to direct the proper management of ventilated trauma patients with OP, and no studies have focussed specifically on these patients. Future randomized trials will need to consider the potential effects of OP on pulmonary mechanics and potential influences on the known risks of ventilator-induced lung injury associated with mechanical ventilation.
Le pneumothorax occulte (PO) se dit d'un pneumothorax que l'examen clinique et la radiographie ordinaire n'ont pas permis de soupçonner mais qui est finalement détecté par tomodensitométrie thoraco-abdominale. Cette situation est de plus en plus courante en traumatologie, étant donné l'utilisation accrue de la tomodensitométrie. Le taux s'établit à environ 5 % chez les traumatisés qui se présentent à l'hôpital, la tomodensitométrie révélant au moins deux fois plus de pneumothorax que la radiographie ordinaire. Le pneumothorax est une cause courante et traitable de mortalité et de morbidité, mais on ne s'entend pas du tout quant au traitement approprié de cette affection. La prise en charge des patients traités aux soins intensifs et ayant besoin de ventilation à pression positive soulève la plus grande controverse. À l'heure actuelle, il n'existe guère de données probantes pour orienter le traitement indiqué des patients traumatisés et ventilés présentant un PO, et aucune étude ne porte particulièrement sur ces patients. Les études cliniques randomisées à venir devront tenir compte des effets éventuels du PO sur le fonctionnement du poumon ainsi que des influences possibles sur les risques connus de lésions pulmonaires provoquées par un ventilateur et subordonnés à la ventilation artificielle.
Figures

References
-
- Blaisdale WF. Pneumothorax and hemothorax. In: Blaisdale WF, Trunkey DD, editors. Trauma management. 3rd ed. New York: Thieme; 1986. p. 150-65.
-
- Richardson JD, Miller FB. Injury to the lung and pleura. In: Felician DV, Moore EE, Mattox KL, editors. Trauma. 3rd ed. Stamford (CT): Appleton & Lange; 1996. p. 387-407.
-
- Stocchetti N, Pagliarini G, Gennari M, Baldi G, Banchini E, Campari M. Trauma care in Italy: evidence of in-hospital preventable deaths. J Trauma 1994;36:401-5. - PubMed
-
- Trupka A, Waydhas C, Hallfeldt KK, Nast-Kolb D, Pfeifer KJ, Schweiberer L. Value of thoracic computed tomography in the first assessment of severely injured patients with blunt chest trauma: results of a prospective study. J Trauma 1997;43:405-12. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous