

Preoperative dexamethasone improves surgical outcome after laparoscopic cholecystectomy: a randomized double-blind placebo-controlled trial
- PMID: 14578725
- PMCID: PMC1356141
- DOI: 10.1097/01.sla.0000094390.82352.cb
Preoperative dexamethasone improves surgical outcome after laparoscopic cholecystectomy: a randomized double-blind placebo-controlled trial
Abstract
Objective: To determine the effects of preoperative dexamethasone on surgical outcome after laparoscopic cholecystectomy (LC).
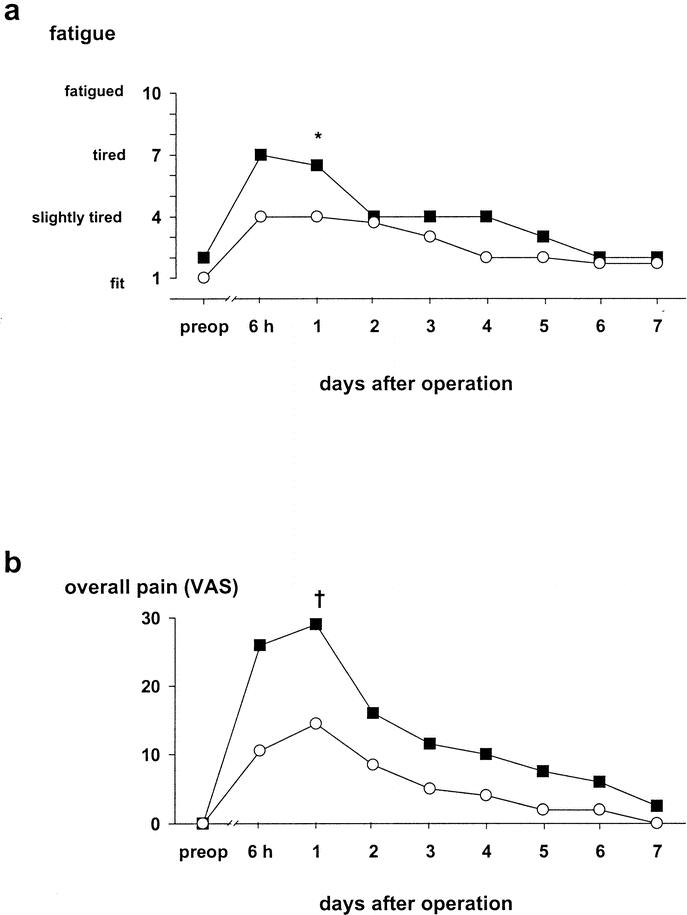
Summary background data: Pain and fatigue are dominating symptoms after LC and may prolong convalescence.
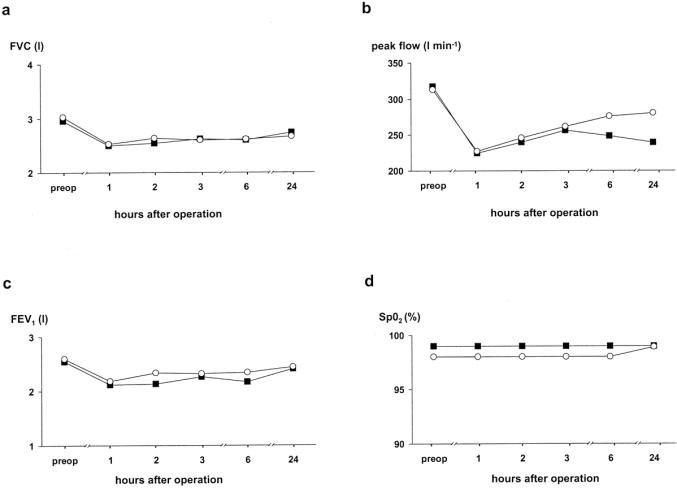
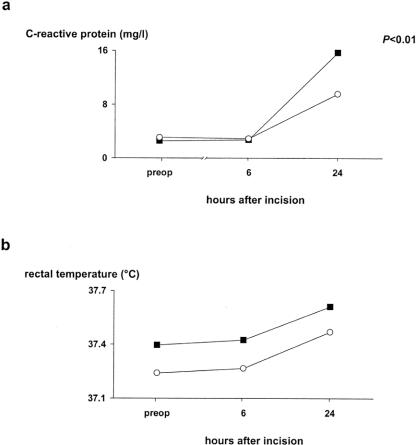
Methods: In a double-blind, placebo-controlled study, 88 patients were randomized to intravenous dexamethasone (8 mg) or placebo 90 minutes before LC. Patients received a similar standardized anesthetic, surgical, and multimodal analgesic treatment. All patients were recommended 2 days postoperative duration of convalescence. The primary endpoints were fatigue and pain. Preoperatively and at several times during the first 24 postoperative hours, we measured C-reactive protein (CRP) and pulmonary function, pain scores, nausea, and number of vomiting episodes were registered. Analgesic and antiemetic requirements were recorded. Also, on a daily basis, patients reported scores of fatigue and pain before and during the first postoperative week and the dates for resumption of work and recreational activities.
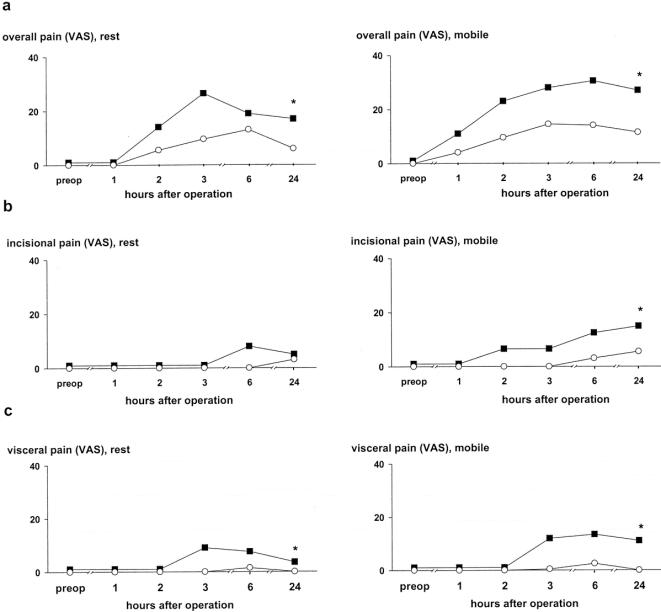
Results: Eight patients were excluded from the study, leaving 40 patients in each study group for analysis. There were no apparent side effects of the study drug. Dexamethasone significantly reduced postoperative levels of CRP (P = 0.01), fatigue (P = 0.01), overall pain, and incisional pain during the first 24 postoperative hours (P < 0.05) and total requirements of opioids (P < 0.05). In addition, cumulated overall and visceral pain scores during the first postoperative week were significantly reduced (P < 0.05). Dexamethasone also reduced nausea and vomiting on the day of operation (P < 0.05). Resumption of recreational activities was significantly faster in the dexamethasone group versus placebo group (median 1 day versus 2 days) (P < 0.05).
Conclusion: Preoperative dexamethasone (8 mg) reduced pain, fatigue, nausea and vomiting, and duration of convalescence in patients undergoing noncomplicated LC, when compared with placebo, and is recommended for routine use.
Figures
Comment in
-
Preoperative steroids for laparoscopic surgery.Ann Surg. 2003 Nov;238(5):661-2. doi: 10.1097/01.sla.0000094391.39418.8e. Ann Surg. 2003. PMID: 14578726 Free PMC article. No abstract available.
References
-
- Johnson A. Laparoscopic surgery. Lancet. 1997;349:631-635. - PubMed
-
- Bisgaard T, Klarskov B, Rosenberg J, et al. Factors determining convalescence after uncomplicated laparoscopic cholecystectomy. Arch Surg. 2001;136:917-921. - PubMed
-
- Bisgaard T, Kehlet H, Rosenberg J. Pain and convalescence after laparoscopic cholecystectomy. Eur J Surg. 2001;167:84-96. - PubMed
-
- Bisgaard T, Klarskov B, Rosenberg J, et al. Characteristics and prediction of early pain after laparoscopic cholecystectomy. Pain. 2001;90:261-269. - PubMed
-
- Sapolsky RM, Romero LM, Munck AU. How do glucocorticoids influence stress responses? Integrating permissive, suppressive, stimulatory, and preparative actions. Endocr Rev. 2000;21:55-89. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
