

Bone marrow failure following severe injury in humans
- PMID: 14578739
- PMCID: PMC1356155
- DOI: 10.1097/01.sla.0000094441.38807.09
Bone marrow failure following severe injury in humans
Abstract
Background: Hematopoietic failure has been observed in experimental animals following shock and injury. In humans, bone marrow dysfunction has been observed in the red cell component and characterized by a persistent anemia, low reticulocyte counts, and the need for repeated transfusions despite adequate iron stores. While a quantitative defect in white blood cell count has not been noted, an alteration in white blood cell function manifesting as an increased susceptibility to infection is well established. Since the etiology of this anemia remains unknown and the bone marrow has been rarely studied following injury, we measured various parameters of hematopoiesis directly using bone marrow from trauma patients and tested the hypothesis that trauma results in profound bone marrow dysfunction, which could explain both the persistent anemia and the alteration in white blood cell function.
Methods: Bone marrow aspirates and peripheral blood were obtained between day 1 and 7 following injury from 45 multiple trauma patients. Normal volunteers served as controls. Peripheral blood was assayed for hemoglobin concentration, reticulocyte count, erythropoietin levels, white blood cell count, and differential. Peripheral blood and bone marrow were cultured for hematopoietic progenitors (CFU-GM, BFU-E, and CFU-E colonies).
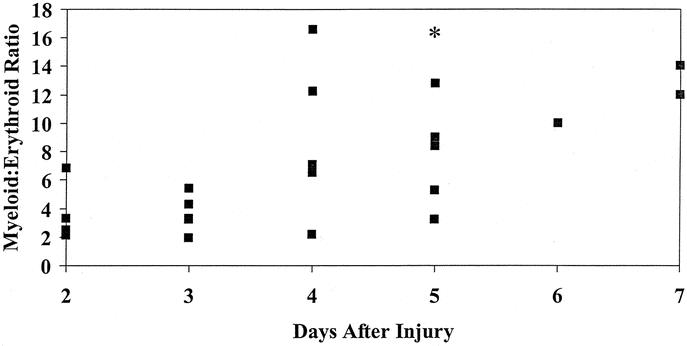
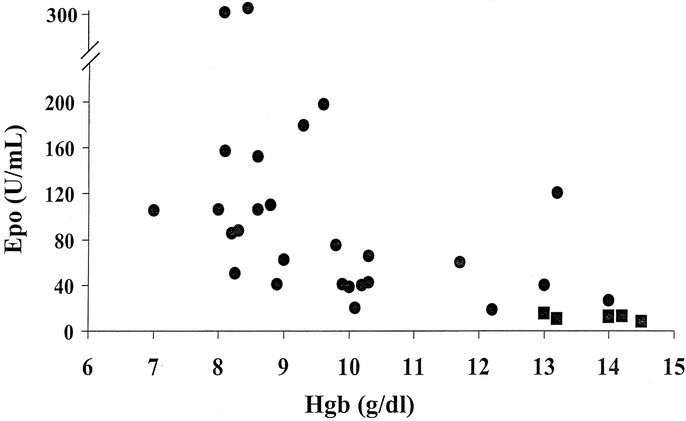
Results: Bone marrow CFU-GM, BFU-E, and CFU-E colony formation was significantly reduced while peripheral blood CFU-GM, BFU-E, and CFU-E was increased in the trauma patients compared with normal volunteers. Bone marrow stroma failed to grow to confluence by day 14 in >90% of trauma patients. In contrast, bone marrow stroma from volunteers always reached confluence between days 10 and 14 in culture. The mean hemoglobin concentration and reticulocyte counts of the trauma patients were 8.6 +/- 1.0 g/dL and 2.75 +/- 0.7% respectively, while their plasma erythropoietin levels were 2 to 10 times greater than control values.
Conclusions: Release of immature white blood cells into the circulation may also contribute to a failure to clear infection and an increased propensity to organ failure. Concomitantly, profound changes occur within the bone marrow, which include the increased release of erythroid and myeloid progenitors into the circulation, a decrease in progenitor cell growth within the bone marrow, and an impaired growth of the bone marrow stroma. Erythropoietin levels are preserved following trauma, implying that the persistent anemia of injury is related to the failure of the bone marrow to respond to erythropoietin.
Figures

References
-
- Baker SP. Injuries: the neglected epidemic: Stone Lecture, 1985 American Trauma Society Meeting. J Trauma. 1987;27:343–348. - PubMed
-
- Moore FA, Haenel JB, Moore EE, et al. Incommensurate oxygen consumption in response to maximal oxygen availability predicts postinjury multiple organ failure. J Trauma. 1992;33:58–67. - PubMed
-
- Heckbert SR, Vedder NB, Hoffman W, et al. Outcome after hemorrhagic shock in trauma patients. J Trauma. 1998;45:545–552. - PubMed
-
- Vaziri N, Eltorai I, Segal J, et al. Erythropoietin profile in spinal cord injured patients. Arch Phys Med Rehabil. 1993;74:65–67. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
