

Review
doi: 10.1016/s0009-9260(03)00308-8.
Imaging in severe acute respiratory syndrome (SARS)
Affiliations
- PMID: 14581005
- PMCID: PMC7176154
- DOI: 10.1016/s0009-9260(03)00308-8
Item in Clipboard
Review
Imaging in severe acute respiratory syndrome (SARS)
Clin Radiol.
2003 Nov.
Abstract
Severe acute respiratory syndrome (SARS) is a highly infectious disease caused by a novel coronavirus, and has become pandemic within a short period of time. Imaging plays an important role in the diagnosis, management and follow-up of patients with SARS. The current status of imaging in SARS is presented in this review.
Figures
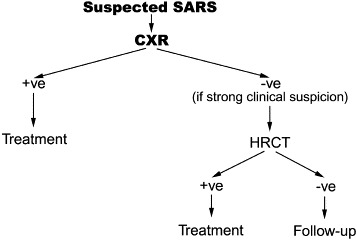
Imaging protocol for suspected case of SARS used at our institution.
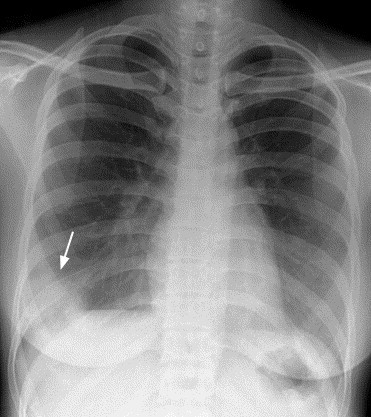
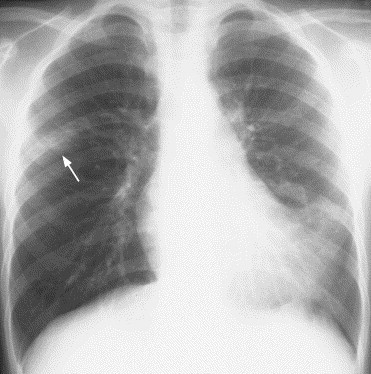
A 26-year-old woman with SARS. Frontal chest radiograph at presentation shows focal ill-defined air-space opacity in periphery of right lower zone (arrow). Note the absence of cavitation, lymphadenopathy and pleural effusion.
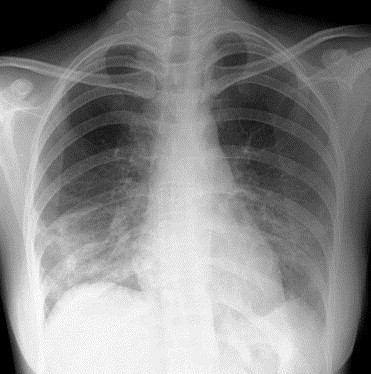
A 26-year-old woman with SARS. Frontal chest radiograph at presentation shows multifocal ill-defined air-space opacities in both lower zones.
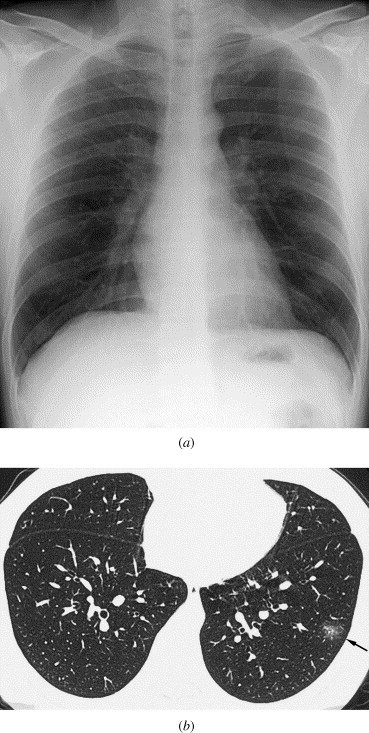
A 36-year-old healthcare worker with SARS. (a) Frontal chest radiograph at presentation is unremarkable. (b) HRCT of the lungs on the same day shows small area of ground-glass opacification in periphery of lateral basal segment of left lower lobe (arrow). HRCT was performed in view of the high clinical index of suspicion and a negative chest radiograph. Subsequent radiographs showed obvious air-space opacification at this site.
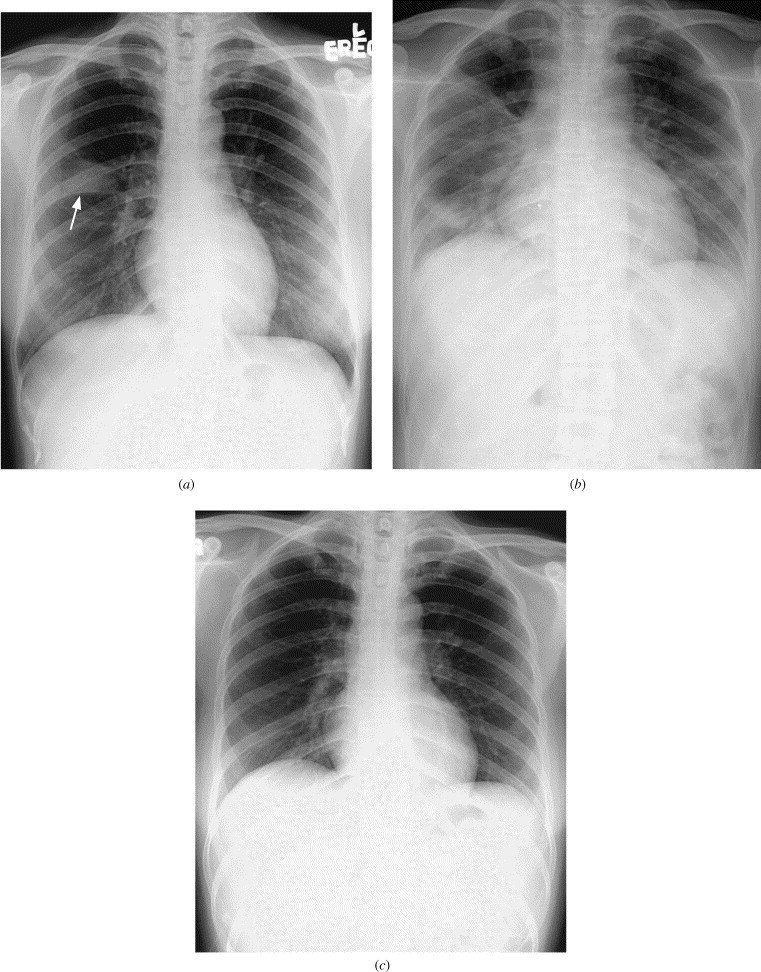
A 45-year-old woman with SARS. (a) Frontal chest radiograph at presentation shows focal segmental air-space opacity in right upper lobe outlining part of horizontal fissure (arrow). (b) Follow-up radiograph 6 days later shows radiographic progression to involve most of right lung and left lower zone. (c) Follow-up radiograph after another 8 days shows near complete resolution of bilateral lung infiltrates after successful therapy.
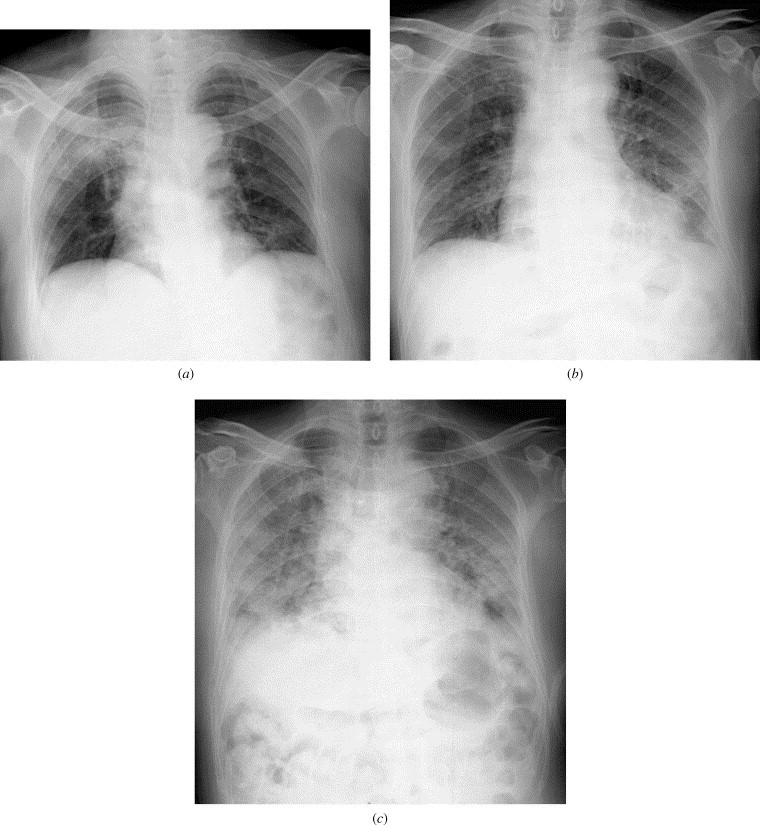
Serial chest radiographs in a 75-year-old man with SARS received medical treatment. (a) Frontal chest radiograph at presentation shows multi-focal ill-defined air-space opacities in right upper zone and to a less extent the left lower zone. (b) Follow-up radiograph 6 days later shows progression of lung infiltrates to the rest of both lungs. (c) Follow-up radiograph after another 4 days shows further radiographic progression to confluent bilateral air-space opacifications simulating acute respiratory distress syndrome (ARDS).
An 8-year-old male patient with SARS. Frontal chest radiograph shows multi-focal ill-defined air-space opacities in left lower zone (obscuring part of left heart border) and periphery of right mid zone (arrow).
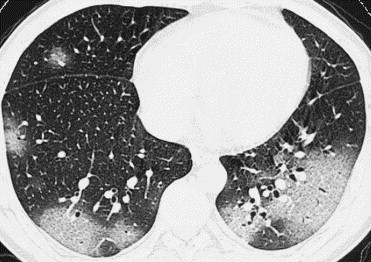
A 29-year-old healthcare worker with SARS. HRCT of thorax (3 days after onset of fever) shows multiple, peripheral, subpleural areas of ground-glass opacification involving both lower and right middle lobes.
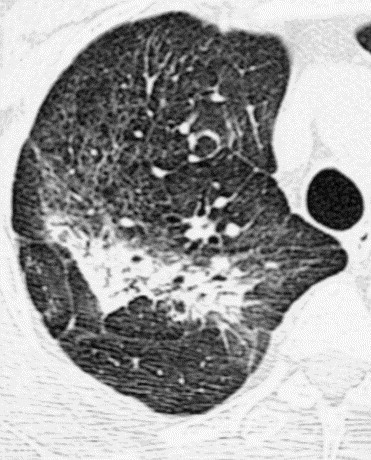
A 39-year-old healthcare worker with SARS and discharged after treatment. HRCT of thorax (8 weeks after initial presentation) shows areas of fibrosis with architectural distortion and traction bronchiectasis in posterior segment of right upper lobe. Interstitial thickening and parenchymal band are also noted in the rest of the right upper lobe.
References
-
- World Health Organisation. Cumulative number of reported probable cases of severe acute respiratory syndrome (SARS) (Accessed May 15, 2003, at http://www.who.int/csr/sars/country/2003_05_14/en/).
-
- Ksiazek T.G, Erdman D, Goldsmith C. A novel coronavirus associated with severe acute respiratory syndrome. N Engl J Med. 2003;348:1953–1966. http://content.nejm.org/cgi/reprint/NEJMoa030781v3.pdf. - PubMed
-
- Drosten C, Gunther S, Preiser W. Identification of a novel coronavirus in patients with severe acute respiratory syndrome. N Engl J Med. 2003;348:1967–1976. - PubMed
-
- World Health Organisation. Case definition of severe acute respiratory syndrome (SARS). (Available at http://www.who.int/csr/sars/casedefinition/en/ Accessed 20 May 2003).
-
- World Health Organisation. Preliminary clinical description of severe acute respiratory syndrome. (Accessed 21 March 2003. http://www.who.int/csr/sars/clinical/en/).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
