

Evaluation of a community-based inner-city disease management program for postmyocardial infarction patients: a randomized controlled trial
- PMID: 14581307
- PMCID: PMC219623
Evaluation of a community-based inner-city disease management program for postmyocardial infarction patients: a randomized controlled trial
Abstract
Background: Disease management programs (DMPs) that use multidisciplinary teams and specialized clinics reduce hospital admissions and improve quality of life and functional status. Evaluations of cardiac DMPs delivered by home health nurses are required.
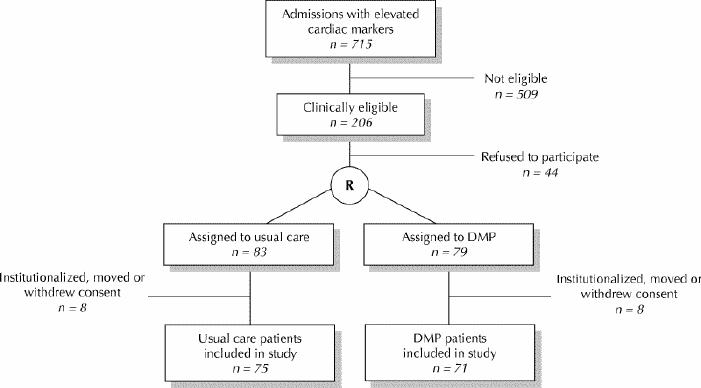
Methods: Between August 1999 and August 2000 we identified consecutive patients admitted to hospital with elevated cardiac enzymes. Patients who agreed were randomly assigned to participate in a DMP or to receive usual care. The DMP included 6 home visits by a cardiac-trained nurse, a standardized nurses' checklist, referral criteria for specialty care, communication with the family physician and patient education. We measured readmission days per 1000 follow-up days for angina, congestive heart failure (CHF) and chronic obstructive pulmonary disease (COPD); all-cause readmission days; and provincial claims for emergency department visits, physician visits, diagnostic or therapeutic services and laboratory services.
Results: We screened 715 consecutive patients admitted with elevated cardiac markers between August 1999 and August 2000. Of those screened 71 DMP and 75 usual care patients met the diagnostic criteria for myocardial infarction, were eligible for visits from a home health nurse and consented to participate in the study. Readmission days for angina, CHF and COPD per 1000 follow-up days were significantly higher for usual care patients than for DMP patients (incidence density ratio [IDR] = 1.59, 95% confidence interval [CI] 1.27-2.00, p < 0.001). All-cause readmission days per 1000 follow-up days were significantly higher for usual care patients than for DMP patients (IDR = 1.53, 95% CI 1.37-1.71, p < 0.001). The difference in emergency department encounters per 1000 follow-up days was significant (IDR = 2.08, 95% CI 1.56-2.77, p < 0.001). During the first 25 days after discharge, there were significantly fewer provincial claims submitted for DMP patients than for usual care patients for emergency department visits (p = 0.007), diagnostic or therapeutic services (p = 0.012) and laboratory services (p = 0.007).
Interpretation: The results provide evidence that an appropriately developed and implemented community-based inner-city DMP delivered by home health nurses has a positive impact on patient outcomes.
Figures
Comment in
-
A disease management program reduced hospital readmission days after myocardial infarction.ACP J Club. 2004 Jul-Aug;141(1):4. ACP J Club. 2004. PMID: 15230552 No abstract available.
References
-
- World Health Organization. Innovative care for chronic conditions: building blocks for action. Geneva: The Organization; 2002.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous