

A meta-analysis comparing the prognostic accuracy of six diagnostic tests for predicting perioperative cardiac risk in patients undergoing major vascular surgery
- PMID: 14594892
- PMCID: PMC1767930
- DOI: 10.1136/heart.89.11.1327
A meta-analysis comparing the prognostic accuracy of six diagnostic tests for predicting perioperative cardiac risk in patients undergoing major vascular surgery
Abstract
Objective: To evaluate the discriminatory value and compare the predictive performance of six non-invasive tests used for perioperative cardiac risk stratification in patients undergoing major vascular surgery.
Design: Meta-analysis of published reports.
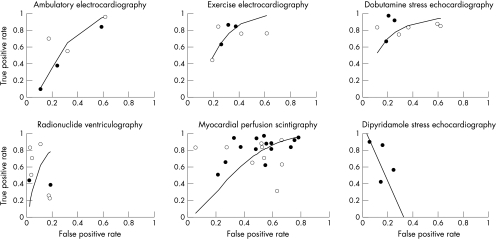
Methods: Eight studies on ambulatory electrocardiography, seven on exercise electrocardiography, eight on radionuclide ventriculography, 23 on myocardial perfusion scintigraphy, eight on dobutamine stress echocardiography, and four on dipyridamole stress echocardiography were selected, using a systematic review of published reports on preoperative non-invasive tests from the Medline database (January 1975 and April 2001). Random effects models were used to calculate weighted sensitivity and specificity from the published results. Summary receiver operating characteristic (SROC) curve analysis was used to evaluate and compare the prognostic accuracy of each test. The relative diagnostic odds ratio was used to study the differences in diagnostic performance of the tests.
Results: In all, 8119 patients participated in the studies selected. Dobutamine stress echocardiography had the highest weighted sensitivity of 85% (95% confidence interval (CI) 74% to 97%) and a reasonable specificity of 70% (95% CI 62% to 79%) for predicting perioperative cardiac death and non-fatal myocardial infarction. On SROC analysis, there was a trend for dobutamine stress echocardiography to perform better than the other tests, but this only reached significance against myocardial perfusion scintigraphy (relative diagnostic odds ratio 5.5, 95% CI 2.0 to 14.9).
Conclusions: On meta-analysis of six non-invasive tests, dobutamine stress echocardiography showed a positive trend towards better diagnostic performance than the other tests, but this was only significant in the comparison with myocardial perfusion scintigraphy. However, dobutamine stress echocardiography may be the favoured test in situations where there is valvar or left ventricular dysfunction.
Figures
References
-
- Mangano DT. Perioperative cardiac morbidity. Anesthesiology 1990;72:153–84. - PubMed
-
- Goldman L, Caldera DL, Nussbaum SR, et al. Multifactorial index of cardiac risk in noncardiac surgical procedures. N Engl J Med 1977;297:845–50. - PubMed
-
- Detsky AS, Abrams HB, McLaughlin JR, et al. Predicting cardiac complications in patients undergoing non-cardiac surgery. J Gen Intern Med 1986;1:211–19. - PubMed
-
- L’Italien GJ, Paul SD, Hendel RC, et al. Development and validation of a Bayesian model for perioperative cardiac risk assessment in a cohort of 1081 vascular surgical candidates. J Am Coll Cardiol 1996;27:779–86. - PubMed
-
- Ouyang P, Gerstenblith G, Furman WR, et al. Frequency and significance of early postoperative silent myocardial ischemia in patients having peripheral vascular surgery. Am J Cardiol 1989;64:1113–16. - PubMed
In appendix
-
- Hanley JA, McNeil BJ. The meaning and use of the area under a receiver operating characteristic (ROC) curve. Radiology 1982;143:29–36. - PubMed
-
- Littenberg B, Moses LE. Estimating diagnostic accuracy from multiple conflicting reports: a new meta-analytic method. Med Decis Making 1993;13:313–21. - PubMed
-
- de Vries SO, Hunink MG, Polak JF. Summary receiver operating characteristic curves as a technique for meta-analysis of the diagnostic performance of duplex ultrasonography in peripheral arterial disease. Acad Radiol 1996;3:361–9. - PubMed
-
- Lijmer JG, Mol BW, Heisterkamp S, et al. Empirical evidence of design-related bias in studies of diagnostic tests. JAMA 1999;282:1061–6. - PubMed
-
- Midgette AS, Stukel TA, Littenberg B.A meta-analytic method for summarizing diagnostic test performances: receiver-operating-characteristic-summary point estimates. Med Decis Making 1993;13:253–7. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous