

Treatment for newly diagnosed hypertension: patterns of prescribing and antihypertensive effectiveness in the UK
- PMID: 14594958
- PMCID: PMC539623
- DOI: 10.1177/014107680309601104
Treatment for newly diagnosed hypertension: patterns of prescribing and antihypertensive effectiveness in the UK
Abstract
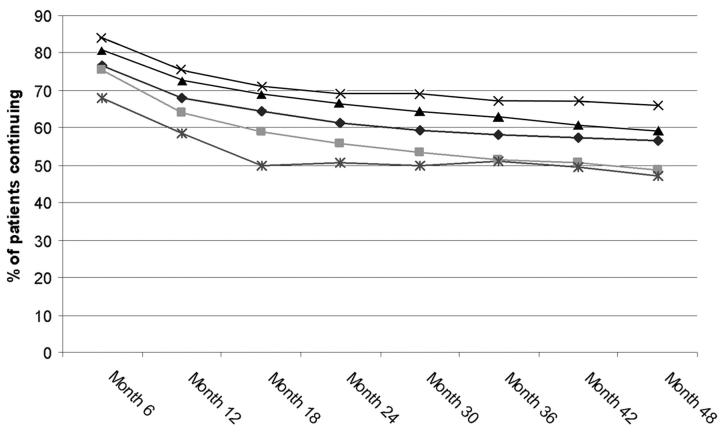
Improved practice in the management of hypertension depends on an understanding of existing patterns of treatment. To describe the management of newly diagnosed hypertension in British general practice and the effectiveness of current prescribing patterns we conducted a retrospective observational study using data from a computerized general practitioner record database (DIN-LINK). 21 024 patients were first treated for newly diagnosed hypertension between January 1993 and December 1997, and were followed for 4 years. Diuretics or beta-blockers were the most widely prescribed first-line treatments, used in 54% of patients. The mean continuation rate for first-line therapy was 69% at 12 months: the continuation rate was highest for angiotensin converting enzyme inhibitors/angiotensin II receptor antagonists. After 12 months of treatment the mean blood pressure reduction was 19/10 mmHg. Blood pressure targets were met in only 14% of patients. After 48 months of treatment 34% of patients had not improved in band of blood pressure severity. Many patients with severe hypertension at 12 months were still being prescribed only one drug. The lack of aggression in antihypertensive treatment, indicated by the low number of agents prescribed and the failure to achieve targets, is disappointing. Prescribing patterns for first-line therapy corresponded to guidelines. Continuation rates on first-line therapy were higher than often reported. The choice of drug for additions to or switches from first-line therapy had no clear pattern. Routinely collected computerized data could be used to support clinical governance activities in primary care.
Figures
Comment in
-
Treatment of hypertension in the UK: simple as ABCD?J R Soc Med. 2003 Nov;96(11):521-2. doi: 10.1177/014107680309601101. J R Soc Med. 2003. PMID: 14594956 Free PMC article. No abstract available.
References
-
- Ramsay L, Williams B, Johnston G, et al. Guidelines for management of hypertension: report of the third working party of the British Hypertension Society. J Hum Hypertens 1999;13: 569-92 - PubMed
-
- Dickerson JE, Hingorani AD, Ashby MJ, Palmer CR, Brown MJ. Optimisation of antihypertensive treatment by crossover rotation of four major classes. Lancet 1999;353: 2008-13 - PubMed
-
- Lip G, Beevers M, Beevers D. The ‘Birmingham Hypertension Square’ for the optimum choice of add-in drugs in the management of resistant hypertension. J Hum Hypertens 1998;12: 761-3 - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
