

Disparities in adolescent health and health care: does socioeconomic status matter?
- PMID: 14596388
- PMCID: PMC1360944
- DOI: 10.1111/1475-6773.00174
Disparities in adolescent health and health care: does socioeconomic status matter?
Abstract
Data collection/extraction methods: National household survey.
Data sources/study setting: We analyzed data on 12,434 adolescents (10 through 18 years old) included in the 1999 and 2000 editions of the National Health Interview Survey.
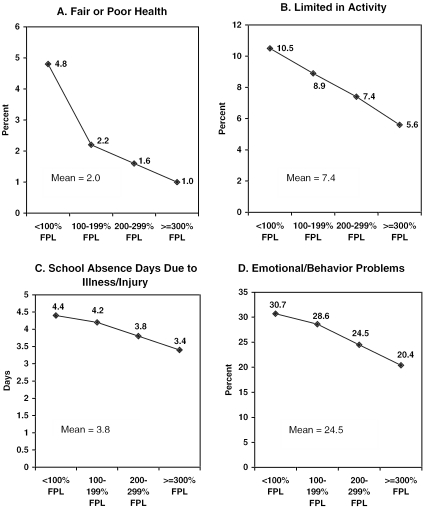
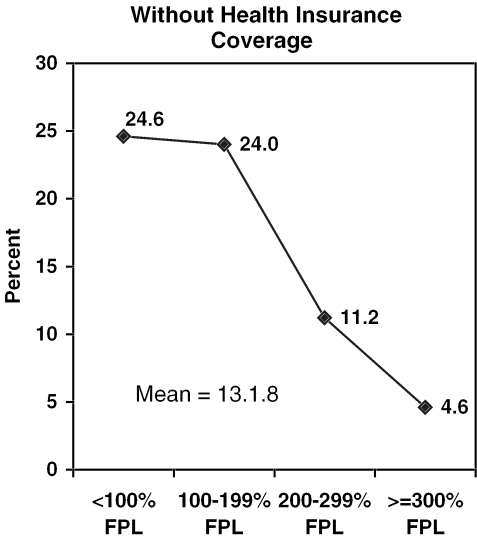
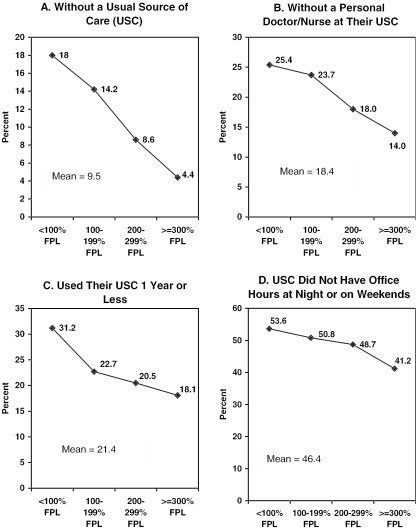
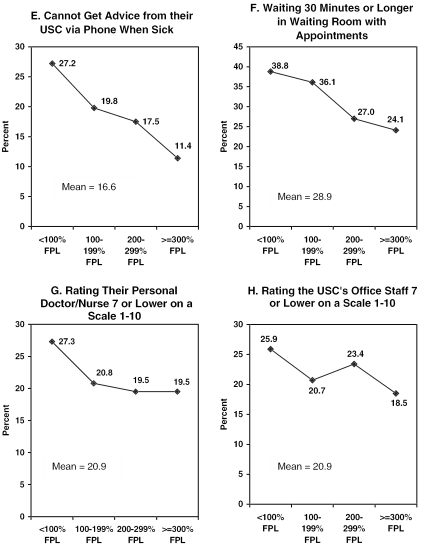
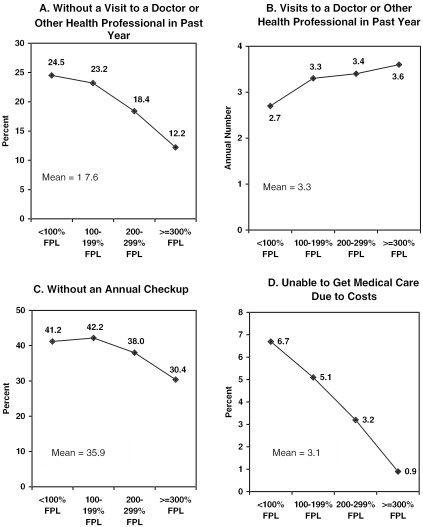
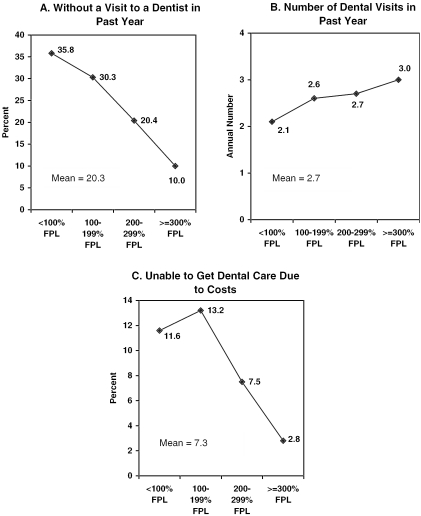
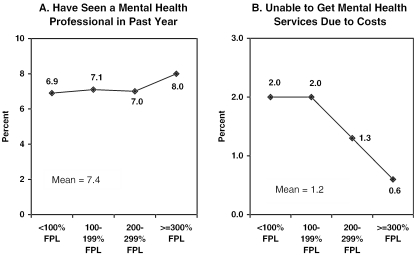
Study design: We assessed the presence of income gradients using four income groups. Outcome variables included health status, health insurance coverage, access to and satisfaction with care, utilization, and unmet health needs.
Principal findings: After adjustment for confounding variables using multivariate analysis, statistically significant disparities were found between poor adolescents and their counterparts in middle- and higher-income families for three of four health status measures, six of eight measures of access to and satisfaction with care, and for six of nine indicators of access to and use of medical care, dental care, and mental health care.
Conclusion: Our analyses indicate adolescents in low-income families remain at a disadvantage despite expansions of the Medicaid program and the comparatively new State Children's Health Insurance Program (SCHIP). Additional efforts are needed to ensure eligible adolescents are enrolled in these programs. Nonfinancial barriers to care must also be addressed to reduce inequities.
Figures
Comment in
-
Socioeconomic status and the fates of adolescents.Health Serv Res. 2003 Oct;38(5):1229-33. doi: 10.1111/1475-6773.00173. Health Serv Res. 2003. PMID: 14596387 Free PMC article. No abstract available.
References
-
- Andersen R, Aday LA. “Access to Medical Care in the U.S.: Realized and Potential.”. Medical Care. 1978;16(4):533–46. - PubMed
-
- Andersen RM. “Revisiting the Behavioral Model and Access to Medical Care: Does It Matter?”. Journal of Health and Social Behavior. 1995;36(3):1–10. - PubMed
-
- Bartman BA, Moy E, D'Angelo LJ. “Access to Ambulatory Care for Adolescents: The Role of a Usual Source of Care.”. Journal of Health Care for the Poor Underserved. 1997;8(2):214–26. - PubMed
-
- Benson V, Marano MA. “Current Estimates from the National Health Interview Survey.”. Vital Health Statistics. 1995;10(199):1–428. - PubMed
-
- Brooks-Gunn J, Duncan G. “The Effects of Poverty on Children.”. Future of Children. 1997;7(2):55–69. - PubMed
