

Using claims data to examine mortality trends following hospitalization for heart attack in Medicare
- PMID: 14596389
- PMCID: PMC1360945
- DOI: 10.1111/1475-6773.00175
Using claims data to examine mortality trends following hospitalization for heart attack in Medicare
Abstract
Objective: To see if changes in the demographics and illness burden of Medicare patients hospitalized for acute myocardial infarction (AMI) from 1995 through 1999 can explain an observed rise (from 32 percent to 34 percent) in one-year mortality over that period.
Data sources: Utilization data from the Centers for Medicare and Medicaid Services (CMS) fee-for-service claims (MedPAR, Outpatient, and Carrier Standard Analytic Files); patient demographics and date of death from CMS Denominator and Vital Status files. For over 1.5 million AMI discharges in 1995-1999 we retain diagnoses from one year prior, and during, the case-defining admission.
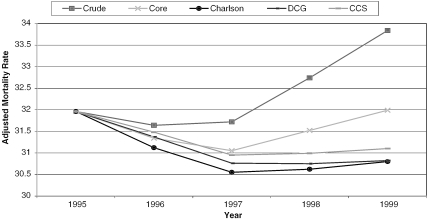
Study design: We fit logistic regression models to predict one-year mortality for the 1995 cases and apply them to 1996-1999 files. The CORE model uses age, sex, and original reason for Medicare entitlement to predict mortality. Three other models use the CORE variables plus morbidity indicators from well-known morbidity classification methods (Charlson, DCG, and AHRQ's CCS). Regressions were used as is--without pruning to eliminate clinical or statistical anomalies. Each model references the same diagnoses--those recorded during the pre- and index admission periods. We compare each model's ability to predict mortality and use each to calculate risk-adjusted mortality in 1996-1999.
Principal findings: The comprehensive morbidity classifications (DCG and CCS) led to more accurate predictions than the Charlson, which dominated the CORE model (validated C-statistics: 0.81, 0.82, 0.74, and 0.66, respectively). Using the CORE model for risk adjustment reduced, but did not eliminate, the mortality increase. In contrast, adjustment using any of the morbidity models produced essentially flat graphs.
Conclusions: Prediction models based on claims-derived demographics and morbidity profiles can be extremely accurate. While one-year post-AMI mortality in Medicare may not be worsening, outcomes appear not to have continued to improve as they had in the prior decade. Rich morbidity information is available in claims data, especially when longitudinally tracked across multiple settings of care, and is important in setting performance targets and evaluating trends.
Figures
References
-
- Ash AS, Moskowitz MA, Speckman J, Franco S, Chaisson C, Posner M, Anderson K, Yacht AC, Caldwell DS. Risk Adjustment Models for Heart Failure. Boston, MA: ResDAC and Boston University School of Medicine; 2001. Report submitted to the Centers for Medicare and Medicaid Services under contract no: 500-96-0023, December.
-
- Ash AS, Posner MA, Chaisson C, Speckman J, Franco S, Yacht AC, Caldwell DS, Moskowitz MA. Risk Adjustment Models to Examine Mortality Trend. Boston, MA: ResDAC and Boston University School of Medicine; 2001. Report submitted to the Centers for Medicare and Medicaid Services under contract no. 500-96-0023, December.
-
- Centers for Medicare and Medicaid Services. (n.d.) National Acute Myocardial Infarction project description, from the Medicare Quality Improvement Community web page [accessed on May 16, 2002]. Available at http://www.medqic.org/content/nationalpriorities/topics/projectdes.jsp?t.... - PubMed
-
- Charlson ME, Pompei P, Ales KL, MacKenzie CR. “A New Method of Classifying Prognostic Comorbidity in Longitudinal Studies: Development and Validation.”. Journal of Chronic Disease. 1987;40(5):373–83. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
