

Tolerability of malaria chemoprophylaxis in non-immune travellers to sub-Saharan Africa: multicentre, randomised, double blind, four arm study
- PMID: 14604928
- PMCID: PMC261741
- DOI: 10.1136/bmj.327.7423.1078
Tolerability of malaria chemoprophylaxis in non-immune travellers to sub-Saharan Africa: multicentre, randomised, double blind, four arm study
Abstract
Objective: To compare the tolerability of malaria chemoprophylaxis regimens in non-immune travellers.
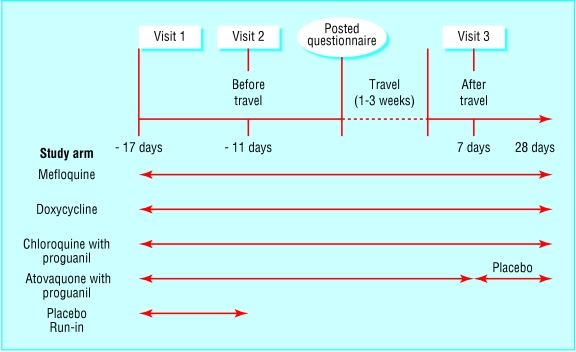
Design: Randomised, double blind, study with placebo run-in phase.
Setting: Travel clinics in Switzerland, Germany, and Israel.
Main outcome measure: Proportion of participants in each treatment arm with subjectively moderate or severe adverse events.
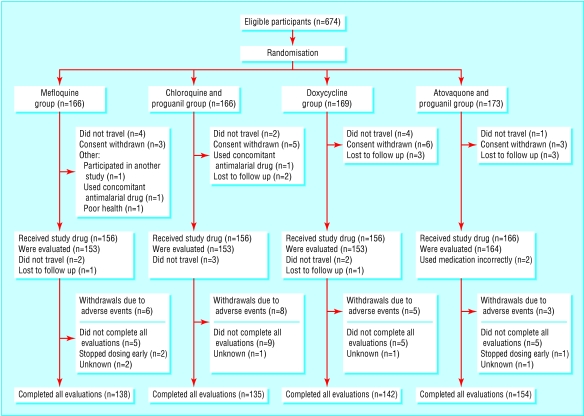
Participants: 623 non-immune travellers to sub-Saharan Africa: 153 each received either doxycycline, mefloquine, or the fixed combination chloroquine and proguanil, and 164 received the fixed combination atovaquone and proguanil.
Results: A high proportion of patients reported adverse events, even in the initial placebo group. No events were serious. The chloroquine and proguanil arm had the highest proportion of mild to moderate adverse events (69/153; 45%, 95% confidence interval 37% to 53%), followed by mefloquine (64/153; 42%, 34% to 50%), doxycycline (51/153; 33%, 26% to 41%), and atovaquone and proguanil (53/164; 32%, 25% to 40%) (P = 0.048 for all). The mefloquine and combined chloroquine and proguanil arms had the highest proportion of more severe events (n = 19; 12%, 7% to 18% and n = 16; 11%, 6% to 15%, respectively), whereas the combined atovaquone and proguanil and doxycycline arms had the lowest (n = 11; 7%, 2% to 11% and n = 9; 6%, 2% to 10%, respectively: P = 0.137 for all). The mefloquine arm had the highest proportion of moderate to severe neuropsychological adverse events, particularly in women (n = 56; 37%, 29% to 44% versus chloroquine and proguanil, n = 46; 30%, 23% to 37%; doxycycline, n = 36; 24%, 17% to 30%; and atovaquone and proguanil, n = 32; 20%, 13% to 26%: P = 0.003 for all). The highest proportion of moderate or severe skin problems were reported in the chloroquine and proguanil arm (n = 12; 8%, 4% to 13% versus doxycycline, n = 5; 3%, 1% to 6%; atovaquone and proguanil, n = 4; 2%, 0% to 5%; mefloquine, n = 2; 1%, 0% to 3%: P = 0.013).
Conclusions: Combined atovaquone and proguanil and doxycyline are well tolerated antimalarial drugs. Broader experience with both agents is needed to accumulate reports of rare adverse events.
Figures
Comment in
-
"Serious" and "severe" adverse drug reactions need defining.BMJ. 2004 Sep 4;329(7465):573. doi: 10.1136/bmj.329.7465.573. BMJ. 2004. PMID: 15345644 Free PMC article. No abstract available.
References
-
- World Health Organization. International travel and health 2002. Geneva: WHO, 2002.
-
- Bradley DJ, Bannister B. Guidelines for malaria prevention in travellers from the United Kingdom for 2001. Commun Dis Public Health 2001;4: 84-101. - PubMed
-
- Centers for Disease Control. Malaria. In: Health information for international travel. Atlanta: US Department of Health and Human Services, 2001.
-
- Committee to Advise on Tropical Medicine and Travel. Canadian recommendations for the prevention and treatment of malaria among international travelers. Ottawa, Canada: Health Canada, 2001. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical