

Tidal volume, cardiac output and functional residual capacity determine end-tidal CO2 transient during standing up in humans
- PMID: 14608002
- PMCID: PMC1664761
- DOI: 10.1113/jphysiol.2003.056895
Tidal volume, cardiac output and functional residual capacity determine end-tidal CO2 transient during standing up in humans
Abstract
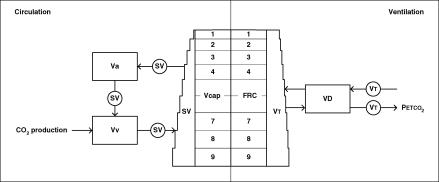
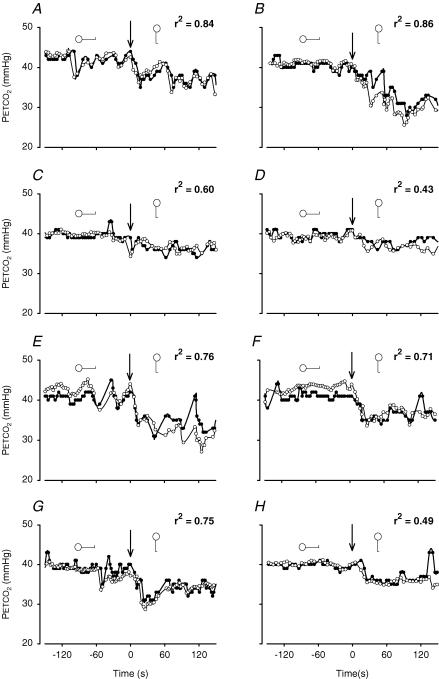
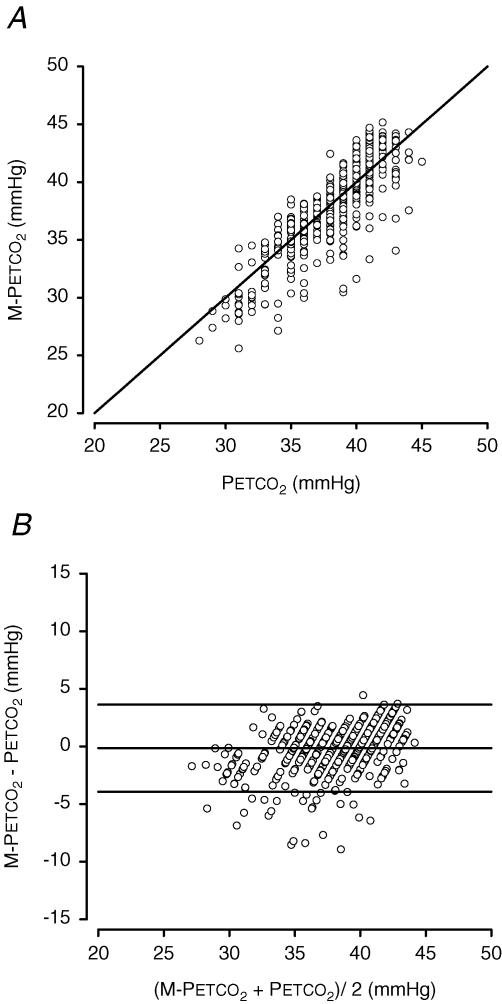
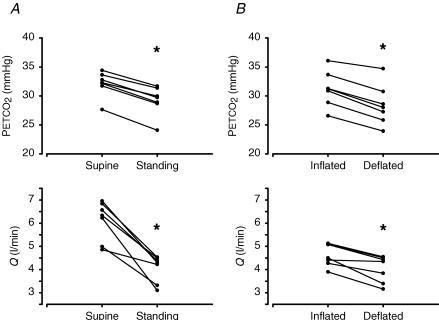
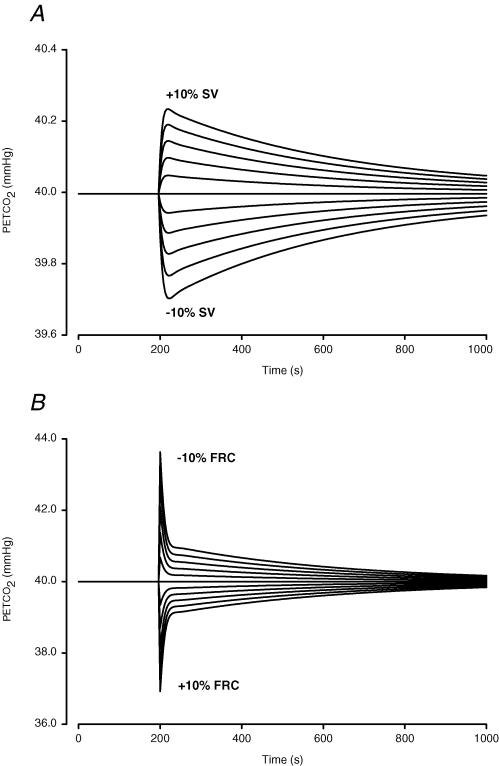
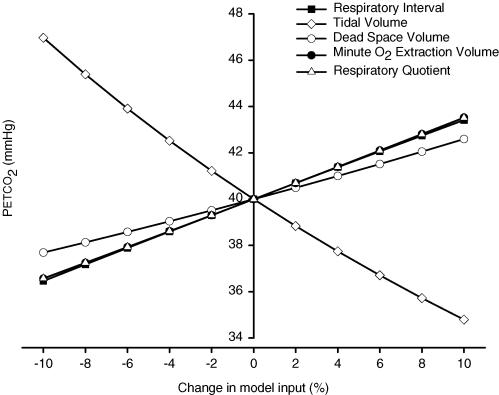
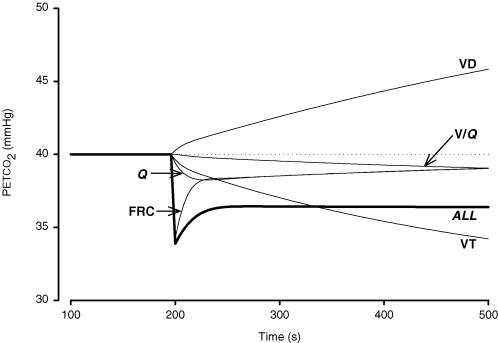
In man assuming the upright position, end-tidal P(CO(2)) (P(ETCO(2))) decreases. With the rising interest in cerebral autoregulation during posture change, which is known to be affected by P(ETCO(2)), we sought to determine the factors leading to hypocapnia during standing up from the supine position. To study the contribution of an increase in tidal volume (V(T)) and breathing frequency, a decrease in stroke volume (SV), a ventilation-perfusion (V/Q) gradient and an increase in functional residual capacity (FRC) to hypocapnia in the standing position, we developed a mathematical model of the lung to follow breath-to-breath variations in P(ETCO(2)). A gravity-induced apical-to-basal V/Q gradient in the lung was modelled using nine lung segments. We tested the model using an eight-subject data set with measurements of V(T), pulmonary O(2) uptake and breath-to-breath lumped SV. On average, the P(ETCO(2)) decreased from 40 mmHg to 36 mmHg after 150 s standing. Results show that the model is able to track breath-to-breath P(ETCO(2)) variations (r(2)= 0.74, P P 0.05). Model parameter sensitivity analysis demonstrates that the decrease in P(ETCO(2)) during standing is due primarily to increased V(T), and transiently to decreased SV and increased FRC; a slight gravity-induced V/Q mismatch also contributes to the hypocapnia. The influence of cardiac output on hypocapnia in the standing position was verified in experiments on human subjects, where first breathing alone, and then breathing, FRC and V/Q were controlled.
Figures
References
-
- Anthonisen NR, Milic-Emili J. Distribution of pulmonary perfusion in erect man. J Appl Physiol. 1966;21:760–766. - PubMed
-
- Birch AA, Dirnhuber MJ, Hartley-Davies R, Iannotti F, Neil-Dwyer G. Assessment of autoregulation by means of periodic changes in blood pressure. Stroke. 1995;26:834–837. - PubMed
-
- Bjurstedt H, Hesser CM, Liljestrand G, Matell G. Effects of posture on alveolar-arterial CO2 and O2 differences and on alveolar dead space in man. Acta Physiol Scand. 1962;54:65–82. - PubMed
-
- Blumenthal SR, Voorhees WD. The relationship between airway carbon dioxide excretion and cardiac output during cardiopulmonary resuscitation. Resuscitation. 1997;34:263–270. - PubMed
-
- Bryan AC, Milic-Emili J, Pengelly D. Effect of gravity on the distribution of pulmonary ventilation. J Appl Physiol. 1966;21:778–784. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical