

Mass antibiotic treatment for group A streptococcus outbreaks in two long-term care facilities
- PMID: 14609461
- PMCID: PMC3033098
- DOI: 10.3201/eid0910.030130
Mass antibiotic treatment for group A streptococcus outbreaks in two long-term care facilities
Abstract
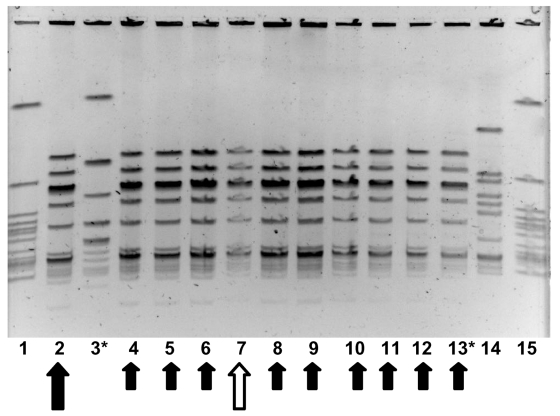
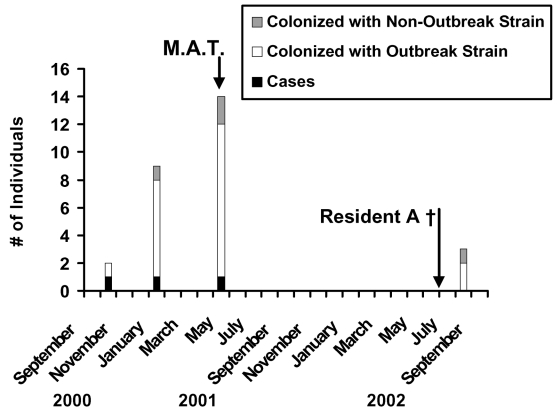
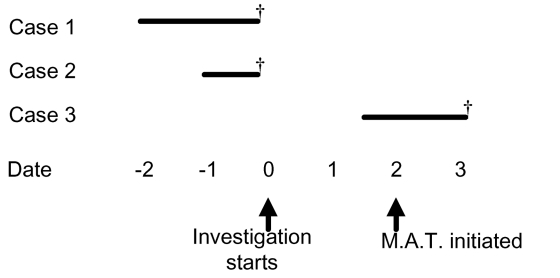
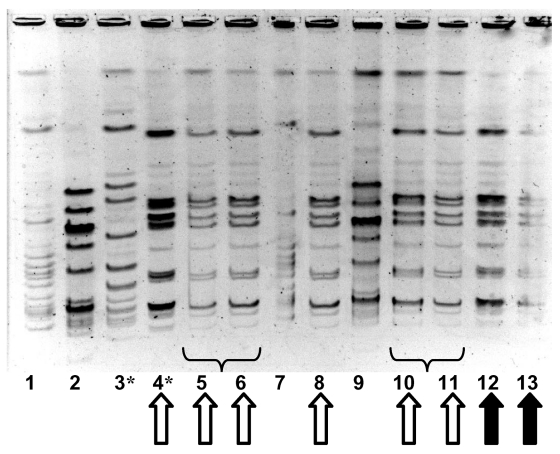
Outbreaks of invasive infections caused by group A β-hemolytic streptococcus (GAS) may occur in long-term care settings and are associated with a high case-fatality rate in debilitated adults. Targeted antibiotic treatment only to residents and staff known to be at specific risk of GAS may be an ineffective outbreak control measure. We describe two institutional outbreaks in which mass antibiotic treatment was used as a control measure. In the first instance, mass treatment was used after targeted antibiotic treatment was not successful. In the second instance, mass treatment was used to control a rapidly evolving outbreak with a high case-fatality rate. Although no further clinical cases were seen after the introduction of mass antibiotic treatment, persistence of the outbreak strain was documented in one institution >1 year after cases had ceased. Strain persistence was associated with the presence of a chronically colonized resident and poor infection control practices.
Figures
Similar articles
-
Group A Streptococcus outbreak among residents and employees of two skilled nursing facilities: North Carolina, 2017.Am J Infect Control. 2019 Jul;47(7):846-849. doi: 10.1016/j.ajic.2018.12.006. Epub 2019 Jan 18. Am J Infect Control. 2019. PMID: 30661909
-
Transmission of group A Streptococcus in long-term care: An outbreak investigation.Am J Infect Control. 2025 Apr;53(4):530-532. doi: 10.1016/j.ajic.2024.11.008. Epub 2024 Nov 20. Am J Infect Control. 2025. PMID: 39577569
-
Mass prophylaxis in an outbreak of invasive group A streptococcal disease in a residential aged care facility.Commun Dis Intell (2018). 2019 May 15;43. doi: 10.33321/cdi.2019.43.18. Commun Dis Intell (2018). 2019. PMID: 31091405
-
Molecular epidemiology and genomics of group A Streptococcus.Infect Genet Evol. 2015 Jul;33:393-418. doi: 10.1016/j.meegid.2014.10.011. Epub 2014 Oct 30. Infect Genet Evol. 2015. PMID: 25460818 Free PMC article. Review.
-
Group A streptococcal outbreaks in nursing homes.Infect Control Hosp Epidemiol. 1992 Dec;13(12):742-7. doi: 10.1086/648348. Infect Control Hosp Epidemiol. 1992. PMID: 1289401 Review. No abstract available.
Cited by
-
Effectiveness and Safety of Antibiotic Prophylaxis for Persons Exposed to Cases of Invasive Group A Streptococcal Disease: A Systematic Review.Open Forum Infect Dis. 2022 May 12;9(8):ofac244. doi: 10.1093/ofid/ofac244. eCollection 2022 Aug. Open Forum Infect Dis. 2022. PMID: 36046698 Free PMC article. Review.
-
Invasive group a streptococcal disease in nursing homes, Minnesota, 1995-2006.Emerg Infect Dis. 2008 May;14(5):772-7. doi: 10.3201/eid1405.070407. Emerg Infect Dis. 2008. PMID: 18439360 Free PMC article.
-
Invasive group A streptococcal infection outbreaks of typeemm118 in a long-term care facility, and of type emm74 in the homeless population, Montréal, Quebec.Can Commun Dis Rep. 2019 Jan 3;45(1):26-31. doi: 10.14745/ccdr.v45i01a03. eCollection 2019 Jan 3. Can Commun Dis Rep. 2019. PMID: 31524888 Free PMC article.
-
Prolonged and large outbreak of invasive group A Streptococcus disease within a nursing home: repeated intrafacility transmission of a single strain.Clin Microbiol Infect. 2019 Feb;25(2):248.e1-248.e7. doi: 10.1016/j.cmi.2018.04.034. Epub 2018 May 18. Clin Microbiol Infect. 2019. PMID: 29783026 Free PMC article.
-
Integration of Genomic and Other Epidemiologic Data to Investigate and Control a Cross-Institutional Outbreak of Streptococcus pyogenes.Emerg Infect Dis. 2016 Jun;22(6):973-80. doi: 10.3201/eid2206.142050. Emerg Infect Dis. 2016. PMID: 27192043 Free PMC article.
References
-
- Kiselica D. Group A beta-hemolytic streptococcal pharyngitis: current clinical concepts. Am Fam Physician. 1994;49:1147–54. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical