

Discontinuation of benzodiazepines among older insomniac adults treated with cognitive-behavioural therapy combined with gradual tapering: a randomized trial
- PMID: 14609970
- PMCID: PMC236226
Discontinuation of benzodiazepines among older insomniac adults treated with cognitive-behavioural therapy combined with gradual tapering: a randomized trial
Abstract
Background: Long-term use of hypnotics is not recommended because of risks of dependency and adverse effects on health. The usual clinical management of benzodiazepine dependency is gradual tapering, but when used alone this method is not highly effective in achieving long-term discontinuation. We compared the efficacy of tapering plus cognitive-behavioural therapy for insomnia with tapering alone in reducing the use of hypnotics by older adults with insomnia.
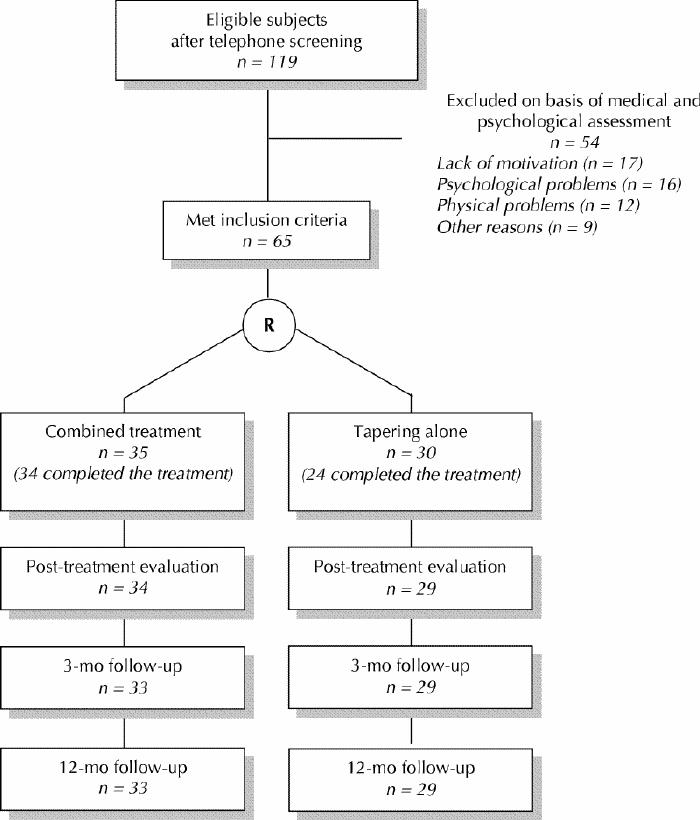
Methods: People with chronic insomnia who had been taking a benzodiazepine every night for more than 3 months were recruited through media advertisements or were referred by their family doctors. They were randomly assigned to undergo either cognitive-behavioural therapy plus gradual tapering of the drug (combined treatment) or gradual tapering only. The cognitive-behavioural therapy was provided by a psychologist in 8 weekly small-group sessions. The tapering was supervised by a physician, who met weekly with each participant over an 8-week period. The main outcome measure was benzodiazepine discontinuation, confirmed by blood screening performed at each of 3 measurement points (immediately after completion of treatment and at 3- and 12-month follow-ups).
Results: Of the 344 potential participants, 65 (mean age 67.4 years) met the inclusion criteria and entered the study. The 2 study groups (35 subjects in the combined treatment group and 30 in the tapering group) were similar in terms of demographic characteristics, duration of insomnia and hypnotic dosage. Immediately after completion of treatment, a greater proportion of patients in the combined treatment group had withdrawn from benzodiazepine use completely (77% [26/34] v. 38% [11/29]; odds ratio [OR] 5.3, 95% confidence interval [CI] 1.8-16.2; OR after adjustment for initial benzodiazepine daily dose 7.9, 95% CI 2.4-30.9). At the 12-month follow-up, the favourable outcome persisted (70% [23/33] v. 24% [7/29]; OR 7.2, 95% CI 2.4-23.7; adjusted OR 7.6, 95% CI 2.5-26.6); similar results were obtained at 3 months.
Interpretation: A combination of cognitive-behavioural therapy and benzodiazepine tapering was superior to tapering alone in the management of patients with insomnia and chronic benzodiazepine use. The beneficial effects were sustained for up to 1 year. Applying this multidisciplinary approach in the community could help reduce benzodiazepine use by older people.
Figures
Comment in
-
Cognitive behavioural therapy improved benzodiazepine discontinuation in chronic insomnia.Evid Based Nurs. 2004 Apr;7(2):52. doi: 10.1136/ebn.7.2.52. Evid Based Nurs. 2004. PMID: 15106632 No abstract available.
-
Cognitive behavioral therapy aided discontinuation of benzodiazepine in chronic insomnia.ACP J Club. 2004 May-Jun;140(3):70. ACP J Club. 2004. PMID: 15122833 No abstract available.
-
Discontinuation of benzodiazepines.CMAJ. 2004 May 25;170(11):1645-6. doi: 10.1503/cmaj.1031869. CMAJ. 2004. PMID: 15159344 Free PMC article. No abstract available.
-
Discontinuation of benzodiazepines.CMAJ. 2004 May 25;170(11):1646. doi: 10.1503/cmaj.1040166. CMAJ. 2004. PMID: 15159347 Free PMC article. No abstract available.
References
-
- Mellinger GD, Balter MB, Uhlenhuth EH. Insomnia and its treatment. Arch Gen Psychiatry 1985;42:225-32. - PubMed
-
- Hohagen F, Käppler C, Schramm E, Rink K, Weyerer S, Riemann D, et al. Prevalence of insomnia in elderly general practice attenders and the current treatment modalities. Acta Psychiatr Scand 1994;90:102-8. - PubMed
-
- Morgan K, Clarke D. Longitudinal trends in late-life insomnia: implications for prescribing. Age Ageing 1997;26:179-84. - PubMed
-
- Henderson S, Jorm AF, Scott R, Mackinnon AJ, Christensen H, Korten AE. Insomnia in the elderly: its prevalence and correlates in the general population. Med J Aust 1995;162:22-4. - PubMed
-
- Ohayon MM, Caulet M. Psychotropic medication and insomnia complaints in two epidemiological studies. Can J Psychiatry 1996;41:457-64. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous