

Epidemiology of paediatric renal stone disease in the UK
- PMID: 14612355
- PMCID: PMC1719348
- DOI: 10.1136/adc.88.11.962
Epidemiology of paediatric renal stone disease in the UK
Erratum in
- Arch Dis Child. 2004 Aug;89(8):797
Abstract
Background: The previous epidemiological study of paediatric nephrolithiasis in Britain was conducted more than 30 years ago.
Aims: To examine the presenting features, predisposing factors, and treatment strategies used in paediatric stones presenting to a British centre over the past five years.
Methods: A total of 121 children presented with a urinary tract renal stone, to one adult and one paediatric centre, over a five year period (1997-2001). All children were reviewed in a dedicated stone clinic and had a full infective and metabolic stone investigative work up. Treatment was assessed by retrospective hospital note review.
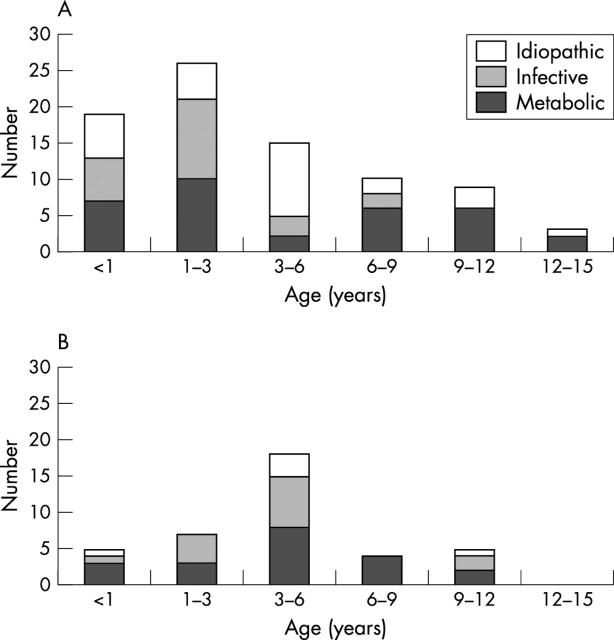
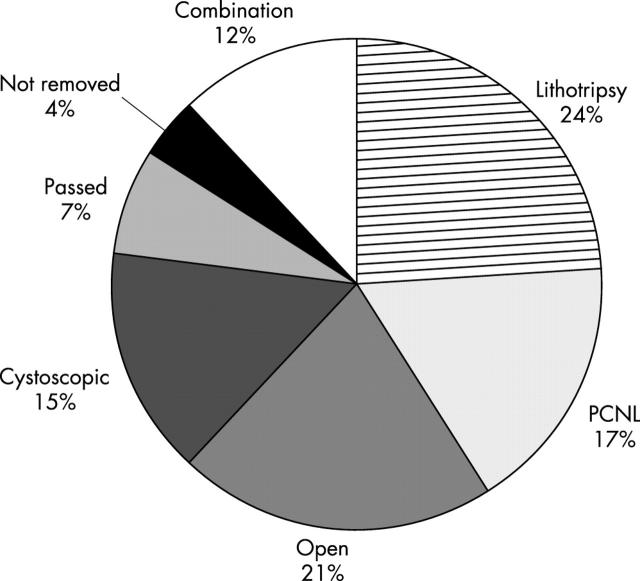
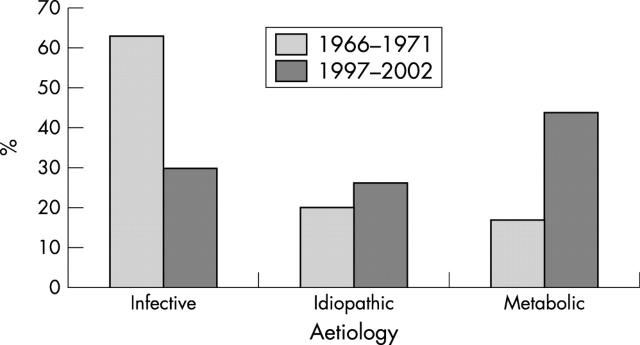
Results: A metabolic abnormality was found in 44% of children, 30% were classified as infective, and 26% idiopathic. Bilateral stones on presentation occurred in 26% of the metabolic group compared to 12% in the infective/idiopathic group (odds ratio 2.7, 95% CI 1.03 to 7.02). Coexisting urinary tract infection was common (49%) in the metabolic group. Surgically, minimally invasive techniques (lithotripsy, percutaneous nephrolithotomy, and endoscopy) were used in 68% of patients.
Conclusions: There has been a shift in the epidemiology of paediatric renal stone disease in the UK over the past 30 years. Underlying metabolic causes are now the most common but can be masked by coexisting urinary tract infection. Treatment has progressed, especially surgically, with sophisticated minimally invasive techniques now employed. All children with renal stones should have a metabolic screen.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous