

Human adipocytes secrete mineralocorticoid-releasing factors
- PMID: 14614137
- PMCID: PMC283571
- DOI: 10.1073/pnas.2336140100
Human adipocytes secrete mineralocorticoid-releasing factors
Abstract
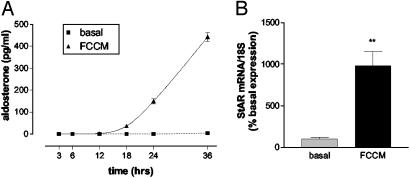
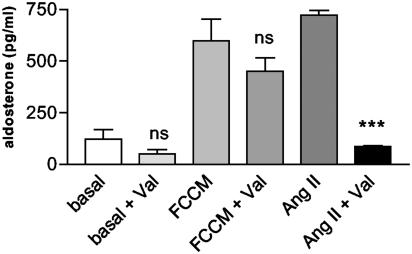
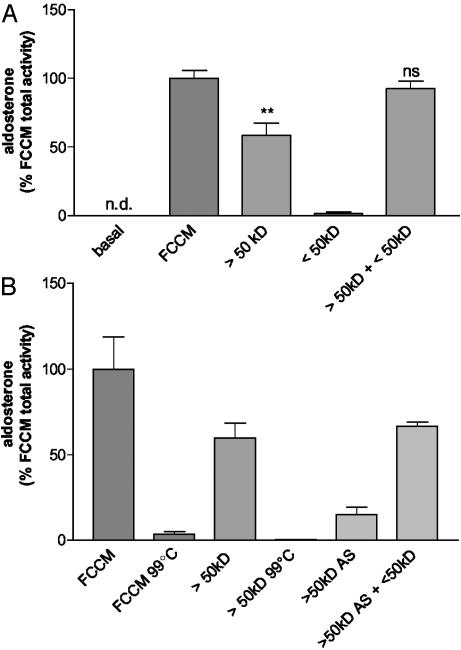
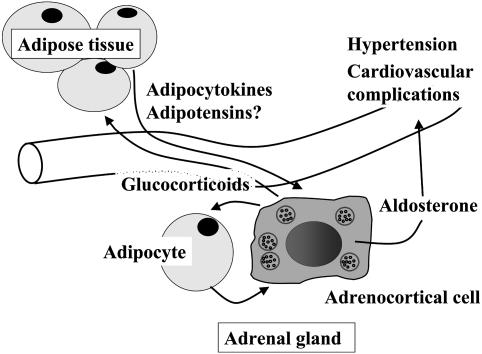
Obesity has become an epidemic problem in western societies, contributing to metabolic diseases, hypertension, and cardiovascular disease. Overweight and obesity are frequently associated with increased plasma levels of aldosterone. Recent evidence suggests that human fat is a highly active endocrine tissue. Therefore, we tested the hypothesis that adipocyte secretory products directly stimulate adrenocortical aldosterone secretion. Secretory products from isolated human adipocytes strongly stimulated steroidogenesis in human adrenocortical cells (NCI-H295R) with a predominant effect on mineralocorticoid secretion. Aldosterone secretion increased 7-fold during 24 h of incubation. This stimulation was comparable to maximal stimulation of these cells with forskolin (2 x 10(-5) M). On the molecular level, there was a 10-fold increase in the expression of steroid acute regulatory peptide mRNA. This effect was independent of adipose angiotensin II as revealed by the stimulatory effect of fat cell-conditioned medium even in the presence of the angiotensin type 1 receptor antagonist, valsartan. None of the recently defined adipocytokines accounted for the effect. Mineralocorticoid-stimulating activity was heat sensitive and could be blunted by heating fat cell-conditioned medium to 99 degrees C. Centrifugal filtration based on molecular mass revealed at least two releasing factors: a heat sensitive fraction (molecular mass >50 kDa) representing 60% of total activity, and an inactive fraction (molecular mass <50 kDa). However, the recovery rate increased to 92% when combining these two fractions, indicating the interaction of at least two factors. In conclusion, human adipocytes secrete potent mineralocorticoid-releasing factors, suggesting a direct link between obesity and hypertension.
Figures

References
-
- World Health Organization (1998) Obesity—Preventing and Managing the Global Epidemic: Report of a WHO Consultation on Obesity (W.H.O., Geneva). - PubMed
-
- Flegal, K. M., Carroll, M. D., Ogden, C. L. & Johnson, C. L. (2002) J. Am. Med. Assoc. 288, 1723–1727. - PubMed
-
- Cameron, A. J., Welborn, T. A., Zimmet, P. Z., Dunstan, D. W., Owen, N., Salmon, J., Dalton, M., Jolley, D. & Shaw, J. E. (2003) Med. J. Aust. 178, 427–432. - PubMed
-
- Kopelman, P. G. (2000) Nature 404, 635–643. - PubMed
-
- Calle, E. E., Rodriguez, C., Walker-Thurmond, K. & Thun, M. J. (2003) N. Engl. J. Med. 348, 1625–1638. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
