

Spinal muscarinic receptors are activated during low or high frequency TENS-induced antihyperalgesia in rats
- PMID: 14614954
- PMCID: PMC2746650
- DOI: 10.1016/s0028-3908(03)00280-6
Spinal muscarinic receptors are activated during low or high frequency TENS-induced antihyperalgesia in rats
Abstract
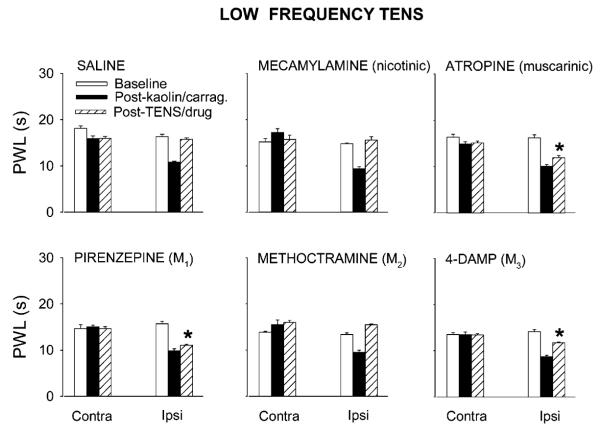
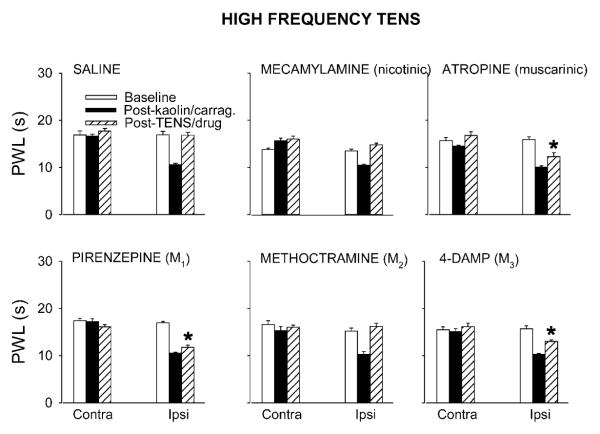
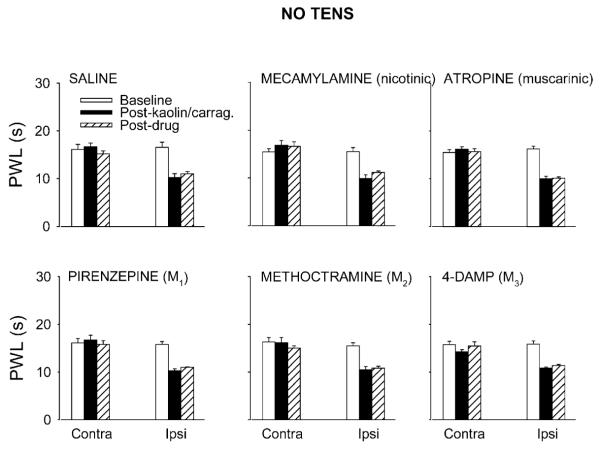
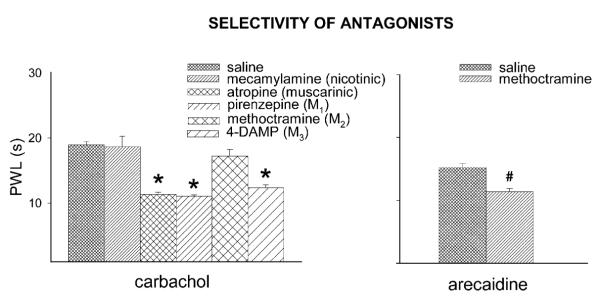
Transcutaneous electrical nerve stimulation (TENS) is a non-pharmacological modality used clinically to relieve pain. Central involvement of serotonin and endogenous opioids are implicated in TENS-induced analgesia. Activation of spinal cholinergic receptors is antinociceptive and these receptors interact with opioid and serotonin receptors. In the current study, the possible involvement of spinal cholinergic receptors in TENS analgesia was investigated in rats. Hyperalgesia was induced by inflaming one knee joint with 3% kaolin-carrageenan and assessed by measuring paw withdrawal latency (PWL) to heat before and 4 h after injection. The non-selective nicotinic antagonist mecamylamine (50 microg), non-selective muscarinic antagonist atropine (30 microg) or one of the muscarinic subtype antagonists: pirenzepine (M1, 10 microg), methoctramine (M2, 10 microg), 4-DAMP (M3, 10 microg), or saline was administered intrathecally just prior to TENS treatment. Low or high frequency TENS was then applied to the inflamed knee and PWL was determined again. Atropine, pirenzepine and 4-DAMP significantly attenuated the antihyperalgesic effects of low and high frequency TENS while mecamylamine and methoctramine had no effects, compared to saline control. The results show that TENS-induced antihyperalgesia is mediated partially by activation of spinal muscarinic receptors but not spinal nicotinic receptors. Further, the results also indicate that spinal M1 and M3 muscarinic receptor subtypes mediate the muscarinic component of TENS antihyperalgesia.
Figures
References
-
- Abelson KS, Hoglund AU. Intravenously administered lidocaine in therapeutic doses increases the intraspinal release of acetylcholine in rats. Neurosci. Lett. 2002;317:93–96. - PubMed
-
- Arimatsu Y, Seto A, Amano T. An atlas of alpha-bungarotoxin binding sites and structures containing acetylcholinesterase in the mouse central nervous system. J. Comp. Neurol. 1981;198:603–631. - PubMed
-
- Borges LF, Iversen SD. Topography of choline acetyltransferase immunoreactive neurons and fibers in the rat spinal cord. Brain Res. 1986;362:140–148. - PubMed
-
- Bouaziz H, Tong C, Eisenach JC. Postoperative analgesia from intrathecal neostigmine in sheep. Anesth. Analg. 1995;80:1114–1140. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
