

Clinical outcome and radiographic results after surgical treatment of post-traumatic thoracolumbar kyphosis following simple type A fractures
- PMID: 14615927
- PMCID: PMC3476569
- DOI: 10.1007/s00586-003-0576-1
Clinical outcome and radiographic results after surgical treatment of post-traumatic thoracolumbar kyphosis following simple type A fractures
Abstract
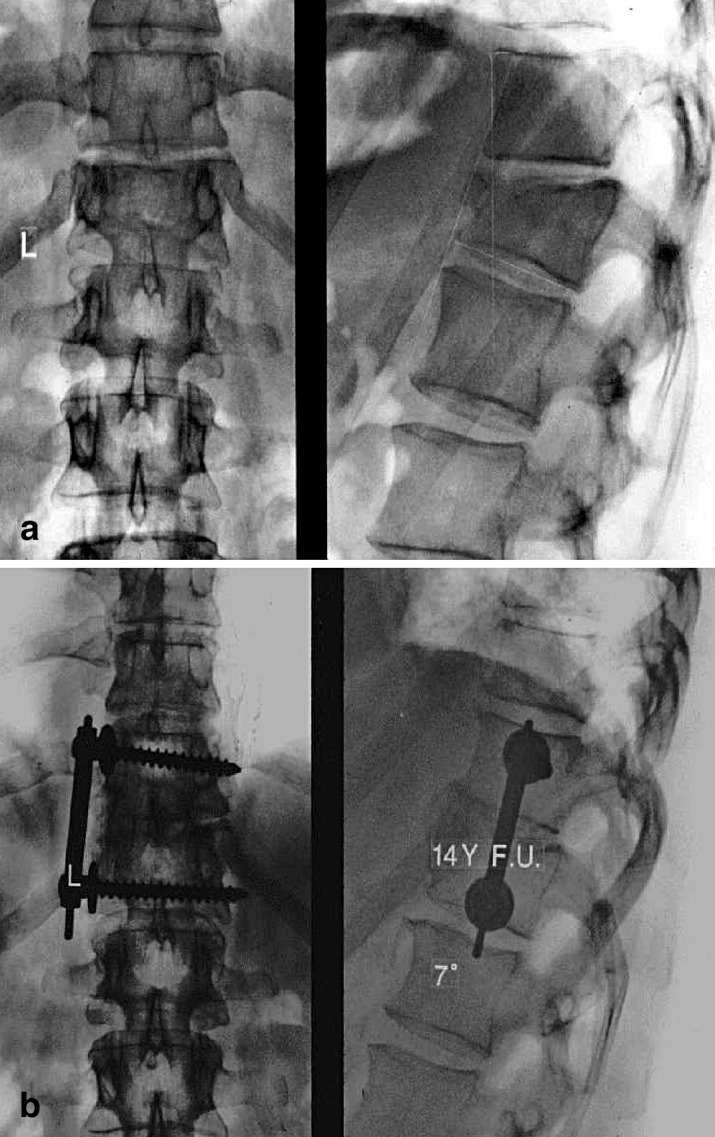
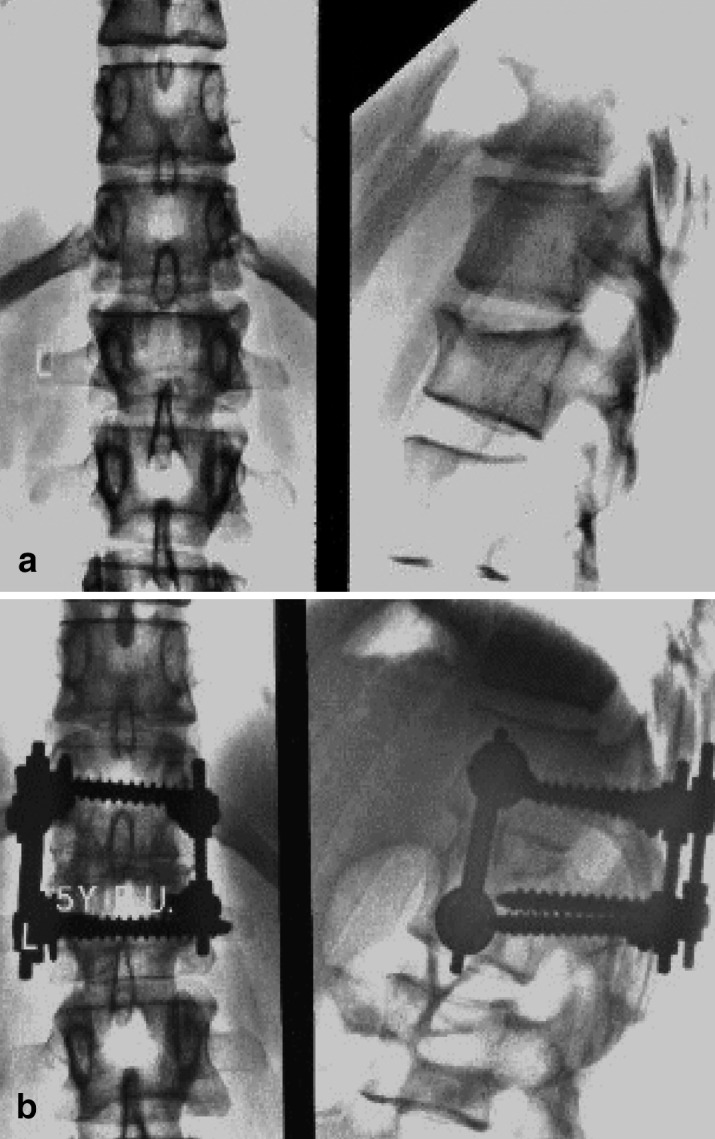
The surgical management of post-traumatic thoracolumbar kyphosis remains controversial. The need for combined procedures is subject to debate, especially for post-traumatic kyphosis after simple type A fractures. The aim of this retrospective study was to evaluate radiographic findings, patient satisfaction and clinical outcome after mono-segmental surgical treatment using an anterior procedure alone (group 1, n = 10 patients) and using a one-stage combined anterior and posterior procedure (group 2, n = 15 patients) for post-traumatic thoracolumbar kyphosis after simple type A fractures. The main indication for surgery was pain. There were no statistically significant differences between the patients in the two groups concerning age, cause of injury, time interval between trauma and surgery, preoperative kyphosis and preoperative back pain score. For all these 25 patients, complete follow-up data were available for retrospective evaluation. The median follow-up was 17 years in group 1 and 8 years in group 2. Radiographic documentation and classification was made on the basis of standing antero-posterior and lateral views and computed tomographic scans. Fractures were categorized according to the Magerl classification. Kyphotic deformity was assessed on lateral radiographs using the Cobb method. Kyphosis angles were measured preoperatively, directly postoperatively, and at final follow-up. For clinical evaluation, the back pain scoring system of Greenough and Fraser was used. Patients were requested to score their status prior to trauma, preoperatively and at follow-up. The Wilcoxon test was used for statistical analysis ( P < 0.05 is significant). In all cases radiographic union was achieved. Median kyphosis in group 1 was corrected from 23 degrees preoperatively to 12 degrees postoperatively ( P < 0.01) and was 11 degrees at follow-up. Median kyphosis in group 2 was corrected from 21 degrees pre-operatively to 12 degrees postoperatively ( P < 0.01) and was 12 degrees at follow-up. The median back score in group 1 changed from 66 points before the trauma to 23 points ( P < 0.01) preoperatively and 35 points at follow-up ( P < 0.01). The median back score in group 2 changed from 67 points before the trauma to 20 points ( P < 0.01) preoperatively and 38 points at follow-up ( P < 0.01). In group 2, four patients had complaints due to annoying prominence of the dorsal instrumentation. In all these cases the dorsal instrumentation was removed. Statistical analysis in this series of ten patients with anterior spondylodesis compared with 15 patients with combined one-stage spondylodesis did not reveal objective advantages of the combined procedure as far as the outcome of radiographic correction of kyphosis or patient outcome is concerned. It is therefore concluded that in cases of post-traumatic thoracolumbar kyphosis after simple type A fractures, mono-segmental correction using an anterior procedure alone, with spondylodesis, is the surgical procedure of choice.
Figures
References
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
